NatureScot Research Report 1338 - Valuing the health and well-being benefits of the NHS outdoor estate in Scotland
Year of publication: 2023
Authors: Alison Holt1, Charles Cowap2, Natalie Johnson1 and Rhiannon Tudor Edwards3
1Natural Capital Solutions, 2Independent consultant, 3Bangor University
Cite as: Holt, A., Cowap, C., Johnson, N. and Tudor Edwards, R. 2023. Valuing the health and well-being benefits of the NHS outdoor estate in Scotland. NatureScot Research Report 1338.
Contents
- Keywords
- Acknowledgements
- Summary
- Conclusions
- Glossary
- 1. Introduction
- 2. Taxonomy of uses of the NHS Scotland outdoor estate
- 3. Assessing health and well-being benefits of the NHS outdoor estate – a conceptual model
- 4. Valuing the health and well-being benefits of the NHS outdoor estate – rapid review and expert panel meeting
- 5. A framework for evaluating and valuing the health and well-being benefits of the NHS Scotland outdoor estate
- 6. Practical application of the framework
- 7. Conclusions and recommendations
- 8. Next steps
- References and Appendices
Keywords
natural capital; health and wellbeing; NHS; outdoor estate; natural capital accounting; tools; ecosystem services
Acknowledgements
The research was commissioned by NatureScot with support from Public Health Scotland. Funding was provided by Scottish Government as part of the programme of work being taken forward to implement the NHS Climate Emergency and Sustainability Strategy 2022-26.
The authors would like to acknowledge and thank Professor Emma McIntosh and Professor Mary Lynch for their contribution on the expert panel. The authors would like to thank Dr Catherine Lawrence for contributing to the final report. The authors would also like to thank Kalpa Pisavadia for production of Figure 5.
Summary
Background
Spending time in green space and access to green space for associated physical exercise, recreation and social networking provides benefits to physical health, mental health and well-being across the life-course. The NHS in Scotland own a considerable outdoor greenspace estate across 14 Health Boards, 7 special Health Boards and Public Health Scotland. The 7 special Health Boards have a special function which covers the whole of Scotland and one public health body which is legally constituted as a Health Board. These are NHS Education for Scotland; Scottish Ambulance Service; NHS National Waiting Times Centre; Healthcare Improvement Scotland; National Services Scotland; NHS 24; The State Hospitals Board for Scotland and Public Health Scotland. It consists of 4.7 million square metres of buildings often part of larger estates rich in greenspace, parks and woodlands. This land is part of the public realm and as institutional ground is, under Scottish Government draft regulations, to be included and considered in local authority open space strategies. This offers opportunities for moving hospitals, health and social care sites from downstream providers of acute and general care to upstream enablers of prevention through the provision of healthy environments and ecosystem services.
The importance of natural capital in delivering such health benefits is recognised by NHS Scotland in its Climate Emergency and Sustainability Strategy (2022-26). The strategy puts forward actions and targets to address climate change impacts, to achieve net zero carbon, and to enhance biodiversity in response to the climate emergency and the need for environmental sustainability, but also recognising that doing so will have a positive impact on human health. Fulfilling these actions will create opportunities for health co-benefits, reduction of health harms and can address health inequalities. It also emphasises NHS Scotland’s role as an anchor organisation, and the strategy sets goals to manage the NHS outdoor estate as a public asset for improvements in public health, and reduction of health inequities.
The opportunity and the challenge
Public Health Scotland and NatureScot have been working with Scottish Health Boards through the Green Exercise Partnership and four NHS Greenspace for Health Partnerships to help deliver infrastructure improvements and activate the outdoor estate. There is also an initiative to create a geospatial data base of the natural capital assets of the NHS Scotland outdoor estate. The remaining challenge is how to identify, measure and value these benefits and the costs of releasing and developing these existing and potential benefits in future. This will inform the opportunity to strengthen the NHS Scotland’s role as an anchor organisation. The aim of this project was to explore the development of a tool or set of tools that can quantify and value the health and well-being benefits related to the use of the NHS outdoor estate.
Our approach
We used a mixed-methods approach to establish a methodology for valuing the health and well-being benefits associated with the NHS outdoor estate. This was achieved through:
- A survey of key personnel in NHS Scotland which has informed an understanding of our proposed taxonomy of uses associated with the NHS outdoor estate.
- The development of a conceptual logic chain of the relationships between natural capital, activities in greenspace, health and well-being benefits and their value.
- A targeted rapid literature review of the scientific and grey literature to reveal metrics of health and well-being benefits and the value from activities akin to those that occur on the NHS outdoor estate.
- A consultation with academic health economists to discuss the appropriateness and robustness of the valuation methods identified in the review, and how NHS Scotland can best approach the valuation of these benefits across the estate and the data required.
Our findings
Survey of uses and users
A survey of uses and users has revealed a wide range of uses and users, although the predominant use across all user categories is walking. Future work could refine this use into the purpose and nature of the activity (e.g. walking in order to travel between buildings v walking as a stretching fitness activity v walking as a necessary component of another activity).
Use can be influenced not only by the natural physical nature of the outdoor estate, but also by facilities and specific initiatives that directly or indirectly support its use. Examples include cycling facilities, not only suitable paths and routes but also secure storage facilities and maintenance equipment. Uses can also be categorised by users and other stakeholders, site characteristics, awareness of potential and other drivers of participation.
The predominant uses identified by respondents included: walking, secure bicycle storage, active travel to and from work, picnic areas, informal recreational gardening, cycling, running, informal social gatherings, outdoor therapeutic interventions or rehabilitation and organised fitness sessions.
The survey has also shown a reasonable level of awareness of the potential of the outdoor estate, with scope to extend this and build on it in securing greater engagement with the outdoor estate. Other organisations, for example local authorities, health and well-being and other charities and local groups, are also involved in the use of the estate, and it should be possible to build on this in the development of future uses of the estate.
Relationships between natural capital and health and well-being
A conceptual model (natural capital logic chain, see below) has been created that describes the pathway to valuing the health and well-being benefits of the NHS outdoor estate.
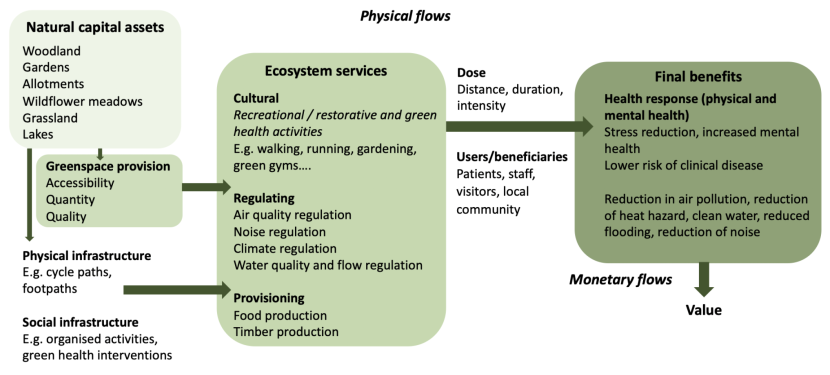
Natural capital logic chain outlining the relationships between natural capital assets, ecosystem services and health and well-being benefits on NHS Scotland outdoor estates
Click for a full description
The above diagram shows the relationships between the natural capital assets (different greenspace types e.g. garden or woodland); the cultural ecosystem services such as recreation or restorative green health activities (e.g. walking, running, birdwatching), and provisioning and regulating services (e.g. air quality, noise and climate regulation) that give rise to health and well-being benefits (increased mental health and happiness, lowering risk of chronic diseases, including health benefits from reducing pollution, noise, heat and flood hazards). It also outlines the beneficiary groups (patients, visitors, staff and local community users) and emphasises that the health and well-being benefits and the regulating service benefits to these groups will vary depending on the type, spatial location, accessibility, quality and quantity of greenspace, the infrastructure that is provided (e.g. cycle paths, footpaths) and organised activities available (e.g. green gyms or practical conservation). All these elements need to be measured to enable a valuation of the natural capital benefits, i.e., the greenspace characteristics as well as the human use and benefits.
The above diagram shows the relationships between the natural capital assets (different greenspace types e.g. garden or woodland); the cultural ecosystem services such as recreation or restorative green health activities (e.g. walking, running, birdwatching), and provisioning and regulating services (e.g. air quality, noise and climate regulation) that give rise to health and well-being benefits (increased mental health and happiness, lowering risk of chronic diseases, including health benefits from reducing pollution, noise, heat and flood hazards). It also outlines the beneficiary groups (patients, visitors, staff and local community users) and emphasises that the health and well-being benefits and the regulating service benefits to these groups will vary depending on the type, spatial location, accessibility, quality and quantity of greenspace, the infrastructure that is provided (e.g. cycle paths, footpaths) and organised activities available (e.g. green gyms or practical conservation). All these elements need to be measured to enable a valuation of the natural capital benefits, i.e., the greenspace characteristics as well as the human use and benefits.
Rapid evidence review
The rapid evidence review was used to find existing metrics that are used to value health and well- being benefits, that would be appropriate for use in the context of the NHS outdoor estate. The focus was placed largely on the cultural services in the review, because there are fewer metrics available at present and it is a fast growing area of research. Regulating services that give rise to health and other benefits are better studied and there are already good metrics available. The searches were limited to research and grey literature published in the English language between 2000-2022. One hundred and sixty-five studies met the inclusion criteria for review. Seventy percent of these papers were focused on quantifying the physical or mental health benefits of activity in a range of greenspaces (e.g. woodland, gardens, parks), and 30% were focused on valuing the benefits from recreational activity, gardening, conservation and ecotherapies.
Overall, the studies quantifying benefits find a positive link between activity in greenspace and an increase in health and well-being, but they are of mixed quality. The largest proportion of the studies focussed on general activities in greenspace, but the second largest on gardens or allotments. The review also demonstrated that there are relatively few studies that have tackled valuing the health and well-being benefits of activities in greenspace. The studies reviewed employ a wide range of valuation methods ranging from the Travel Cost Method (TCM), Contingent Valuation (CVM) and Willingness to Pay (WTP) to QALYs, DALYs and Social Return On Investment (SROI). This suggests that a broad range of valuation methods are applicable. The review has provided some scope for transferring these benefits to the NHS outdoor estate cases, but only in very particular circumstances.
Proposed building blocks framework for evaluation and valuation of health and well-being benefits
Following a meeting with three leading experts in the field of Health Economics we have proposed a “building blocks” framework for the evaluation and valuation of the health and well-being benefits from the NHS outdoor estate. The framework provides a pathway towards a robust assessment of the benefits, ensuring that these benefits are considered fairly alongside other priorities in NHS estate business cases. The framework has been constructed recognising the importance of time-horizons in public health and preventative interventions. Many benefits to physical and mental health and the life-time health opportunity architecture of the population involve costs now and benefits many years in the future. It, therefore, encompasses short term metrics of e.g. greenspace use, as well as methods that will capture the longer term benefits. The framework is also place-based in accordance with guidance in the HM Treasury Green Book, which is linked to the concept of NHS estates as anchor organisations recognising the social, economic and environmental factors that help create good health within local neighbourhoods, playing a key role in addressing health inequalities. The framework supports that the NHS Scotland outdoor estate move from downstream providers of care to upstream preventers of ill-health and disability.
The framework is designed to capture qualitative and quantitative (non-monetary) valuation of the health and well-being benefits so they can be used in decision-making, recognising that it won’t be possible to estimate a monetary value for all of these benefits, and that monetary valuation is only one way of capturing these benefits. It takes a realist valuation approach understanding that socio- economic factors will impact on whether a green health intervention will work. It integrates the natural capital accounting approach and a novel health economics approach to measuring health and well-being benefits from the natural environment (borrowing methods from environmental economics).
The framework is an integrated and modular approach consisting of three steps:
- Step 1 uses a cost consequence framework that captures costs and impacts associated with the outdoor estate activities and interventions. This aligns with guidance from the National Institute for Health and Care Excellence (NICE) for the evaluation of public health interventions which emphasises the appropriateness of cost consequence and cost benefit analysis, taking a wider intersectoral perspective on the identification, measurement and valuation of costs and benefits.
- Step 2 uses a social cost benefit, social return on investment (SROI) framework, centred on the NHS outdoor estate, for evaluating and valuing the benefits associated with it, using the Treasury Green Book as a benchmark.
- Step 3 is concerned with the prioritisation of competing demands at the whole estate level using multi-criteria decision analysis, for the assessment of competing demands on NHS estates.
Practical application of the framework
Data
Greenspace assets: Any approach to valuation will require data on each element (natural capital assets, ecosystem services (cultural, regulating and provisioning) and final benefits) of the conceptual model of the relationships between natural capital assets and health and well-being benefits outlined above. The spatial database of the outdoor greenspace at each of the Health Boards is key to understanding the potential to supply health and well-being benefits. This will aid assessments of quantity, quality and accessibility of these greenspaces and how it influences patient, staff and local community use. This is understanding supply in relation to demand both by physical location, but also considering the social and economic reasons that may make sites accessible and attractive or not. NHS estates will have to be carefully managed for the range of different uses and user groups. A spatial analysis of the greenspaces could inform zoning of the outdoor estate within larger sites. Data on the types of users attracted to the estate greenspaces could be gathered as part of an annual survey of well-being benefits related to greenspace (see below).
Use: Data is required on how the site is being used (e.g. gardening, walking, green gym, outdoor therapeutic interventions, bird watching etc) and by whom. We recommend a survey of use, by different zones at sites throughout the year, and a register of organised health interventions recording the numbers of participants involved in the activity. There are innovative technologies that can help monitor use (e.g. counters on footpaths and cycle paths, sensors on benches, innovative smartphone apps).
Health and well-being benefits: There is a requirement for primary data collection across a range of activities to understand the uses and benefits associated with the NHS greenspace beneficiaries, rather than using existing studies for benefits transfer (the available valuation studies are generally at the wrong scale and too generic for robust benefits transfer to the NHS outdoor estate). However, benefits transfer may be appropriate for specific green health interventions, such as therapeutic gardening, where activities are very similar and take place at a similar scale. Understanding the benefits and their value is, therefore, contingent on gathering data by survey. A well designed annual survey of well-being related to greenspace is recommended. This should also be used to gather important data on the users, such as user type (patient, staff, visitor or local user), gender, ethnicity and socio-economic circumstances. Spotting the gaps in users will enable NHS boards to take appropriate action to establish equality of accessibility.
The health and well-being benefits associated with the provisioning and regulating services can be captured using benefits transfer as in natural capital accounting. A good guide for economic methods is provided in the Defra ENCA ecosystem services data book.
Where to start?
Capturing the value of all the possible health and well-being benefits, across all activities and beneficiaries associated with NHS Scotland’s outdoor estate will be challenging. Consequently, it is sensible to focus initially on using the proposed framework to evaluate situations where there are relatively easy wins, while data is gathered for dealing with the rest. We suggest an initial focus on staff health and well-being (mental and musculoskeletal health), and some specific green health interventions (e.g. gardening and social and green prescribing) in relation to all users.
We also suggest testing out the framework on some pilot NHS Health Board sites and focusing on gathering data as recommended with a focus on different user groups, benefit types and green health interventions (as above) to create learning that can be rolled out across all the Health Boards. This will generate data on benefits transfer that can more easily be applied to other NHS estates.
Conclusions
There is no quick route to valuing the health and well-being benefits of the NHS outdoor estate in a robust way. There may be some quick wins using benefits transfer from other studies for specific organised health activities where there are known numbers of participants, or from very generic recreational activities in specific habitats (such as walking in woodland).
Primary studies using surveys will be necessary to quantify and value health and well-being benefits across a range of NHS outdoor estate activities. The most efficient use of resources would be to prioritise certain activities or user groups and run different projects on pilot NHS Health Board sites. The learning can then be applied to other sites and be used in a future valuation toolkit in the medium to long term.
Summary of recommendations
We recommend the following for a robust evaluation and valuation of the health and well-being benefits from the use of the NHS outdoor estate. They will also help NHS Scotland develop their role as an anchor institution, allowing the outdoor estate to contribute to prevention of illness and address health inequalities:
- Adopt a place-based approach with an awareness of the opportunities being different for urban and rural estate.
- Be aware of time-horizons for valuation and the role of discount rates.
- Employ a shift in thinking about hospitals and their estate as places of acute care to places with a role to play in prevention.
- Begin to gather data and monitor use of the green estate.
- Employ the proposed building blocks framework to valuation.
- An initial focus on benefits to the NHS workforce addressing mental and musculoskeletal health.
- Establish the concept of zoning the green estate for staff, for patients and visitors, for green parking, and for community activities using green estate land.
- Establish demonstration sites with built-in evaluation and the resources required for evaluation with outside links to those familiar with methods evaluation of costs and benefits.
- Deliver evaluations including academic publication in peer-reviewed journals as well as accessible web-based reports and infographics.
- Work collaboratively with experts in the field.
Glossary
| Term | Definition |
|---|---|
| Anchor organisation | An organisation which has an important presence in a place and is tied to a particular place through mission, physical assets and local relationships. Key to this is that the institution is tied to the well-being of the population and influences community health and well-being. Implicit from an NHS perspective is that the NHS has a responsibility to deliver community benefits through the way it operates. |
| B£ST | Benefits Estimation Tool. |
| Biodiversity | An abbreviation of ‘Biological diversity’. The variability among living organisms from all sources including, inter alia, terrestrial, marine and other aquatic ecosystems and the ecological complexes of which they are part; this includes diversity within species, between species and of ecosystems. |
| Boolean operators | Words like “and” and “not” which allow expansion of search parameters. |
| CBA | Cost-Benefit Analysis. |
| CCA | Cost-Consequence Analysis. |
| CEA | Cost-Effectiveness Analysis. |
| CICES v5.1 | Common International Classification for Ecosystem Services. |
| Cultural services | Non-material benefits that can be obtained from ecosystems, such as physical health and well-being and spiritual enjoyment. |
| CVM | Contingent Valuation Method. |
| DALY | Disability Adjusted Life Year. |
| DCE | Discrete Choice Experiment. |
| Ecosystem service | The direct and indirect contributions of ecosystems to human well-being and quality of life. There are four categories of ecosystem services: Provisioning, Regulating, and Cultural. The term ‘services’ is usually used to encompass the tangible and intangible benefits that humans obtain from ecosystems, which are sometimes separated into ‘goods’ and ‘services.’ |
| Ecosystem service flow /physical flow | The flow of ecosystem services provided by natural capital e.g. tonnes of carbon sequestered or number of recreational visits. |
| GIS | Geographical Information Systems. |
| GI-Val | Green Infrastructure Valuation Toolkit. |
| Green parking | Semi-paved car parks that provide sustainable drainage, prevent the movement of soil and clogging up of sewer systems. Recycled materials are often used. |
| Habitat condition | The Biodiversity Metric V.3.1 uses habitat condition as one of the measures of habitat quality. It measures the variation in the quality of patches of the same habitat type against ecological optimum state for that particular habitat. |
| HALY | Health Adjusted Life Years. |
| HEAT | Health Economic Assessment Tool. |
| ICECAP | ICEpop CAPability Measure. |
| InVEST | Integrated Valuation of Ecosystem Services and Trade-Offs. |
| Likert scale | A rating scale used in surveys to gauge opinions, values or perceptions. Respondents choose from given options and the responses can then be given a numerical score for numerical analysis. Invented in 1932 by Rensis Likert, America social psychologist (1903-1981). |
| Local climate regulation | The capacity of habitats / natural capital assets to cool the local environment and cause a reduction in urban heat maxima. |
| Logic chain | A natural capital logic chain shows the links between natural capital assets (their quantity, quality and location) and the ecosystem services and benefits they provide. |
| MCDA | Multi-Criteria Decision Analysis. |
| Monetary flow | The monetary value of the benefits that flow from natural capital assets. |
| Natural capital | Elements of nature that directly or indirectly produce value or benefits to people, including ecosystems, species, freshwater, land, minerals, the air and oceans, as well as natural processes and functions. |
| Natural capital accounting | Natural capital accounting is the use of an accounting framework to provide a systematic way to measure and report on the value of the stocks of natural capital and flows of ecosystem service benefits. It documents the natural capital assets, the physical flows of ecosystem services and the monetary flows (or value) of the benefits. It provides a net natural capital value by accounting for liabilities associated with maintaining the natural capital assets. This term is often confused with natural capital assessment, or the monetary valuation of ecosystem service benefits. |
| Natural capital assessment | Describing or quantifying natural capital assets, the benefits that flow from them and their value. Can include opportunities analysis for restoring or creating new habitat for enhancing the delivering of benefits. Provides natural capital evidence for integration into decision-making to improve natural capital management. |
| Natural capital assets | A distinctive component or grouping of natural capital components, including e.g. habitats, soils and air. |
| Natural capital stock | The store of natural capital assets on which humans depend (amount of freshwater, grassland or woodland etc). |
| NEVO | Environment Valuation Online. |
| NICE | National Institute for Health and Care Excellence. |
| Noise attenuation | The capacity of the land to diffuse and absorb noise pollution. Noise can impact health, well-being, productivity and the natural environment. |
| ORVal | Outdoor Recreation Valuation. |
| PAMS | Property and Asset Management Strategies. |
| Present value | Today's value of the benefits you expect to flow from a natural capital asset in the future. |
| Provisioning services | Characterised by the products obtained from ecosystems such as food, water and timber. |
| QALY | Quality-Adjusted Life Years. |
| Qualitative assessment | The descriptive and conceptual findings of non-numerical data. |
| Quantitative assessment | The collection and analysis of numerical data. |
| Regulating services | Any benefit obtained from the natural processes and functioning of ecosystems such as flood reduction, water quality, pollination or carbon sequestration. |
| Sensitivity analysis | A tool to evaluate the impacts of different assumptions and possible outcomes of a valuation. |
| Spatial data | Data that references a specific geographical area or location. |
| SROI | Social Return on Investment. |
| TCM | Travel Cost Method. |
| VOSL | Value of a Statistical Life. |
| WELLBY | Well-Being Adjusted Life Year. |
| WTA | Willingness To Accept. |
| WTP | Willingness To Pay. |
1. Introduction
Access to green space and associated physical exercise, recreation and social networking provide benefits to physical health, mental health and well-being across the life-course. The NHS in Scotland own a considerable outdoor greenspace estate across 14 Health Boards, 7 special Health Boards and Public Health Scotland. The 7 special Health Boards have a special function which covers the whole of Scotland and one public health body which is legally constituted as a Health Board. These are NHS Education for Scotland; Scottish Ambulance Service; NHS National Waiting Times Centre; Healthcare Improvement Scotland; National Services Scotland; NHS 24; The State Hospitals Board for Scotland and Public Health Scotland. It consists of 4.7 million square metres of buildings often part of larger estates rich in greenspace, parks and woodlands (Scottish Government, 2022a). This land is part of the public realm and as institutional ground is, under Scottish Government draft regulations, to be included and considered in Local Authority Open Space Strategies. This offers opportunities for moving hospitals from downstream providers of acute care to upstream enablers of prevention through the provision of healthy environments and ecosystem services.
Contact with nature, and specific nature-based or green health interventions, can deliver health benefits to patients, visitors, NHS staff and local communities. The importance of natural capital in delivering such health benefits is recognised by NHS Scotland in its Climate Emergency and Sustainability Strategy (2022-26) (Scottish Government, 2022a). The strategy puts forward actions and targets to address climate change impacts, to achieve net zero carbon, and to enhance biodiversity in response to the climate emergency and the need for environmental sustainability. This is alongside fulfilling its duty as a public body to deliver on biodiversity (Nature Conservation (Scotland) Act 2004) and contribute to meeting the climate change target of net zero by 2045 (Climate Change (Scotland) Act 2009). However, importantly in this context the strategy also recognises that fulfilling these actions will create opportunities for health co-benefits, reduce health harms and address health inequalities.
The strategy also emphasises NHS Scotland’s role as an anchor organisation. There is a need for the significant land and physical assets of NHS Scotland to contribute a positive influence on the social, economic and environmental factors that help create good health within local neighbourhoods, playing a key role in addressing health inequalities (Reed et al., 2019). NHS Scotland as an anchor organisation is a specific focus of the Place and Well-being programme within the Scottish Government’s Care and Well-Being Portfolio (Scottish Government, 2022b), and links to the Public Health Scotland Place and Well-being Outcomes (Public Health Scotland, 2022).
NatureScot along with Scottish Forestry, NHS Health Scotland and NHS National Services Scotland has been working with Scottish Health Boards through the Green Exercise Partnership to deliver infrastructure improvements and set up four NHS Greenspace for Health Partnerships to improve activation of the NHS estate. Public Health Scotland are currently creating a geospatial data base of the natural capital assets of the NHS Scotland estate. The remaining challenge is how to identify, measure and value the health and well-being benefits that the NHS outdoor estate generates, and the costs of releasing and developing these existing and potential benefits in future. NatureScot and Public Health Scotland would like to develop a tool or set of tools that can quantify and value these benefits. The aims of the project were to:
- Review the variety of existing uses of the NHS physical outdoor estate in Scotland for health and well-being benefit.
- Complete a rapid literature review of existing Natural Capital Assessment approaches or tools that include a health and well-being component relevant to urban developments as well as rural settings that would be appropriate within health care sites and services in Scotland.
- Provide recommendations on the appropriateness and robustness of these specific health and well-being approaches or tools.
- Devise a simple ‘Phase 1’ conceptual model that sets out the relationships between the natural capital assets of a greenspace, the ecosystem services that are derived from those assets, the beneficiaries of those ecosystem services and the health and well-being outcomes experienced by those beneficiaries.
- Recommend the inputs (the data) that will be needed for a tool to support the evaluation and valuation of the health and well-being benefits of NHS greenspace and the indicative costs of collecting/ collating that data.
- Recommend the outputs that will be needed from a tool to support the evaluation and valuation of the health and well-being benefits of NHS Greenspace.
This report first presents the results of the survey of uses and users that has informed a taxonomy of uses associated with the NHS outdoor estate (Section 2), it then sets out a conceptual logic chain of the relationships between natural capital, ecosystem services and the health and well-being benefits that need to be considered for valuation (Section 3). This is followed by the results of a rapid review of metrics used to quantify and value the health and well-being benefits akin to those that might occur from the NHS outdoor estate (Section 4). In Section 5 we propose a framework for evaluating and valuing the health and well-being benefits flowing from the NHS outdoor estate and explain the concepts that underpin this approach. The following section (Section 6) then outlines how this framework can be put into practice across the estates, outlining the data requirements that will take the NHS Health Boards closer to being able to value the health and well-being benefits, measures that are required for improving access, and areas to focus efforts to achieve greatest impact and quick wins. The conclusions and recommendations from this project are presented in Section 7, followed by suggestions for next steps for the broader initiative (Section 8).
2. Taxonomy of uses of the NHS Scotland outdoor estate
The work described in this section focuses on the development of a survey to capture current uses and users of the NHS Scotland outdoor estate. Preliminary semi-structured interviews were undertaken with NHS staff who were able to offer key interests and/or experience in this area. Information from these interviews was synthesised with findings from the literature review to develop an online survey for wider distribution through NHS Scotland.
2.1. The interviews
Online interviews were undertaken via Teams and Zoom on four occasions with eleven Health Service staff from a range of functions and regions. The outcomes of these discussions have been instrumental in identifying perspectives on the use of NHS greenspace for therapeutic and other purposes, the importance of strategic placement, the role of other agencies, bodies and organisations in catalysing green space initiatives and in identifying previous initiatives which, although discontinued in a number of cases, continue to be valuable sources of insight. We have also identified uses of greenspace which had not previously appeared in our background research.
2.2. The survey
The objective of the survey was to fill a gap in our knowledge about the extent and types of use and user on the NHS Scotland outdoor estate, focused on health and well-being benefits. The first steps in designing the survey drew on the literature review, in particular the identification of different uses and users identified across a selection of academic and grey literature.
The survey was initially designed on paper, reviewed with the project steering group and subsequently modified for delivery by LimeSurvey, the designated software for this project. Further modifications were then made in the light of initial online testing before the survey went fully live.
The questions in the survey covered:
- Respondent familiarity with the use of the NHS outdoor estate in Scotland for health and well- being purposes.
- Respondent relationship to the estate, as an NHS employee, volunteer or other user.
- The NHS Scotland Board or Boards referred to in respondents’ answers.
- Identification of existing uses, activities and facilities.
- Identification of uses according to the different user groups: Patients, Staff, Volunteers, Visitors, Local community uses and others.
- Extent or intensity of use according to NHS functional areas (for example medical speciality).
- Involvement of other organisations, focussed on local authorities, health and welfare charities, national agencies like the Forestry Commission, conservation and similar charities, local groups distinguishing those with a health focus, special interest, children and youth, early years.
- The extent to which health and well-being benefits of the outdoor estate are recognised within Property and Asset Management Strategies.
The survey went live on 27 February 2023, with a request for responses by 6 March.
By 8th March, 200 complete responses had been received and these were drawn for analysis. Distribution of the survey was by email to NHS contacts with requests to distribute the survey link to further contacts. This does mean that we do not know how many potential respondents were contacted, nor anything about the nature of a population for sampling purposes. Nevertheless, we do have a profile of the responses we have received in terms of their self-perceived familiarity with the use of the NHS outdoor estate for health and well-being, and their role in relation to the NHS outdoor estate and the Scottish Health Board or Boards their answers relate to. Figures 1a, b & c provide summaries of these responses.
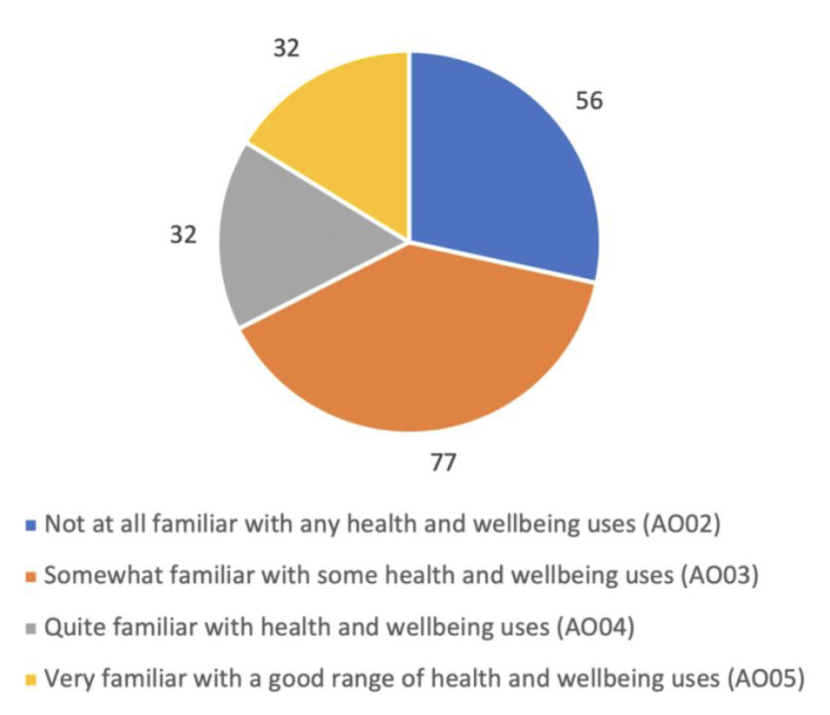
Figure 1a. Numbers of respondents to the question: How familiar do you feel you are with the use of the NHS outdoor estate in Scotland for health and well-being purposes?
Click for a full description
Figure 1a is a pie chart showing the responses of 197 people to the question “How familiar do you feel you are with the use of the NHS outdoor estate in Scotland for health and well-being purposes?” Of those respondents, 56 were not at all familiar with any health and wellbeing uses, 77 were somewhat familiar with some health and wellbeing uses, 32 were quite familiar with health and wellbeing uses and 32 were very familiar with a good range of health and wellbeing uses. Therefore most respondents were not at all familiar or merely somewhat familiar with the health and well-being benefits associated with use of the NHS estate in Scotland.
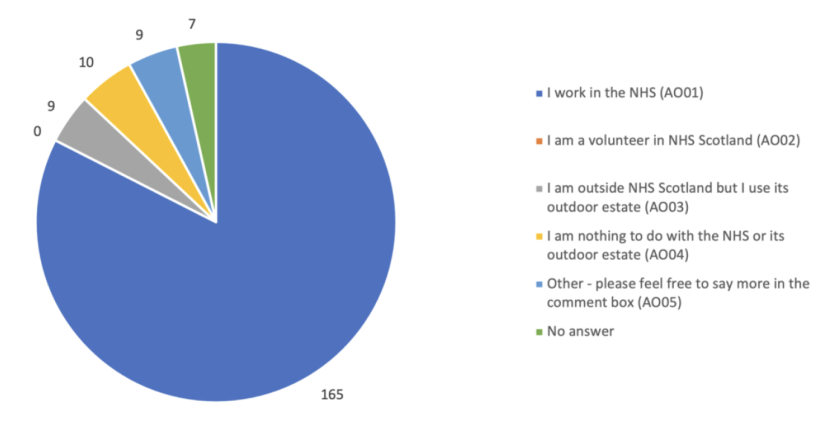
Figure 1b. Respondent (number) perspective on the NHS outdoor estate.
Click for a full description
Figure 1b a is a pie chart showing the status of the 200 respondents to the questionnaire in relation to the NHS estate.165 of the respondents worked in the NHS. 9 did not work for the NHS but used the outdoor estate, 10 had nothing to do with the NHS or its outdoor estate. Most respondents (83%) work in the NHS. No volunteers responded.
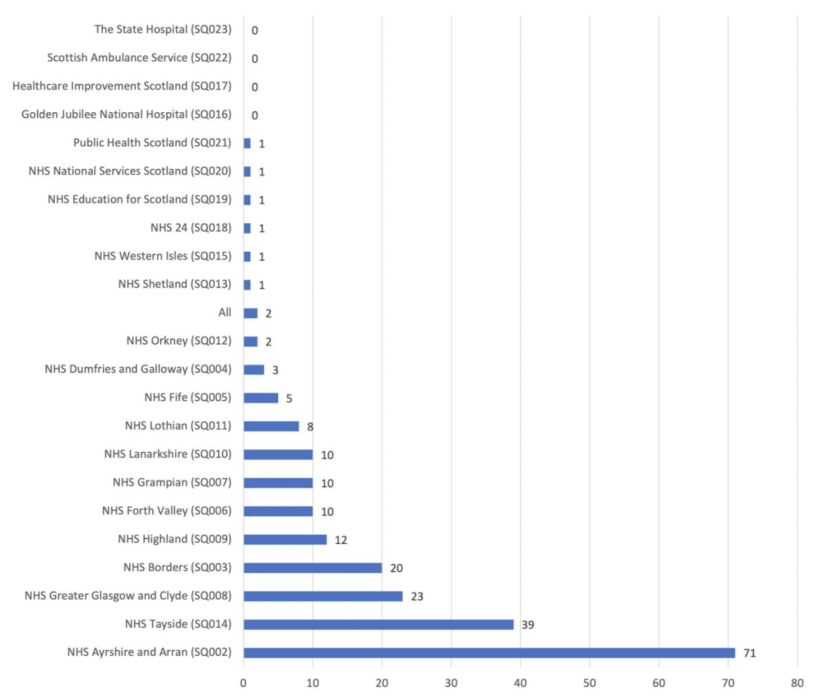
Figure 1c. The Board or Boards your answers refer to (number of respondents).
Click for a full description
Figure 1 c is a bar chart showing the responses of 221 respondents to a question that asked for the Health Board or Boards on which respondents had based their answers. 71 respondents had based their answers on NHS Ayrshire and Arran, and NHS Tayside accounted for 39 of the responses. Together these Boards accounted for half the responses. NHS Greater Glasgow and Clyde accounted for 23 or the responses, NHS Borders accounted for 20, NHS Forth Valley accounted for 10, as did NHS Grampian and NHS Lanarkshire. NHS Lothian accounted for 8 and NHS Fife accounted for 5. No responses were received from the Golden Jubilee National Hospital, Healthcare Improvement Scotland, Scottish Ambulance Service and The State Hospital.
Most survey respondents were not at all familiar or merely somewhat familiar with the health and well-being benefits associated with use of the NHS estate in Scotland (133 of 200 respondents, Figure 1a). Most respondents (165/200, 83%) work in the NHS. No volunteers responded. There were small numbers in the remaining categories in the survey (see Figure 1b).
There were 221 responses to the question that asked for the Health Board or Boards on which respondents had based their answers (Figure 1c). NHS Ayrshire and Arran dominated, and along with NHS Tayside accounted for half the responses (110 responses of 221). At the other end of this scale, no responses were received from the Golden Jubilee National Hospital, Healthcare Improvement Scotland, Scottish Ambulance Service and The State Hospital. This may represent an onward distribution bias when considering the results in view of the snowballing approach whereby the survey was initially distributed to all boards.
Table 1 lists the uses, activities and facilities identified by respondents in rank order. Walking and secure bicycle storage were the two most prominent uses according to the number of respondents who identified each, followed by active travel to and from work (itself likely to be by walking or cycling – categories were not mutually exclusive).
Oddly secure bicycle storage was identified by 106 respondents, but cycling itself by only 55 respondents. Uses of a therapeutic nature included:
- Outdoor therapeutic interventions or rehabilitation – recognised by 21% of respondents, and ranked 9th.
- This was followed by Organised Fitness Sessions – 20% of respondents and rank 10th. It is not possible to tell directly from the responses whether the organised fitness sessions were set up with a medical therapeutic intention.
We also sought to distinguish uses by different groups: patients, staff, volunteers, visitors and others. Respondents chose from a shorter list of activities and their responses are presented in Table 2, with uses presented in rank order for each group. Not surprisingly walking is the highest ranked activity on each list, but there is then considerable variation between groups. The value of this information may be in enabling the selection of activities for further development and promotion according to local user priorities.
Table 3 summarises the intensity of use within different NHS functional areas, for example psychiatry, obstetrics, occupational health (a total of 18 higher order divisions of the work of the NHS). The functional areas were based on NHS workforce development groupings with some modification to avoid confusion in the light of steering group feedback. The overwhelming answer for all functional areas was that respondents did not know.
The Stand-Out groups in Table 3 are Health Promotion, Psychiatry, Occupational Health and Primary Care. This is based on the total number of responses in the two highest categories in the Likert scale used for this question. The Likert scale itself is reproduced in Table 3. One respondent stated that every NHS Functional Area made extensive use of the outdoor estate for therapeutic, medical or other service purposes including active use or promotion in treatment pathway plans with active monitoring of outcomes. This is not credible, and this response could be removed for future analysis. Nevertheless, its inclusion does not affect the relative position of the functional areas. Clearly some functional areas will struggle ever to make more than a minimal use of the outdoor estate for therapeutic or medical purposes, and these results may be helpful in supporting the top users to increase their use and share with others, and to encourage the next tier of users as to how they might engage more fruitfully with the NHS outdoor estate.
We were also interested in the involvement of other organisations in health and well-being activities on the estate. Table 4 summarises the results of this section of the survey.
| Answer | Count | Percentage |
|---|---|---|
| Walking (SQ002) | 157 | 78.50% |
| Secure bicycle storage (SQ010) | 106 | 53.00% |
| Active travel to/from work (SQ019) | 75 | 37.50% |
| Picnic areas (SQ018) | 72 | 36.00% |
| Informal recreational gardening (SQ013) | 69 | 34.50% |
| Cycling (SQ005) | 55 | 27.50% |
| Running (SQ004) | 49 | 24.50% |
| Informal social gatherings (SQ036) | 43 | 21.50% |
| Outdoor therapeutic interventions or rehabilitation (SQ024) | 42 | 21.00% |
| Organised fitness sessions (SQ009) | 40 | 20.00% |
| Meetings (SQ025) | 39 | 19.50% |
| Active travel within estate (SQ020) | 38 | 19.00% |
| Organised social exercise eg walking or wheeling club (SQ022) | 37 | 18.50% |
| Nature conservation tasks eg tree planting or hedge laying (SQ026) | 37 | 18.50% |
| Communal bicycle repair facility (SQ012) | 35 | 17.50% |
| Visual arts display eg statues (SQ029) | 34 | 17.00% |
| Artistic creation eg drawing and painting (SQ028) | 33 | 16.50% |
| Teaching and learning (SQ017) | 31 | 15.50% |
| Wheeling (SQ003) | 30 | 15.00% |
| Bicycle hire/loan (SQ011) | 29 | 14.50% |
| Community Food production (SQ015) | 26 | 13.00% |
| Informal play (SQ007) | 25 | 12.50% |
| Birdwatching or other wildlife study (SQ032) | 23 | 11.50% |
| Formally organised social gatherings (SQ037) | 21 | 10.50% |
| Outdoor exercise equipment eg green gym (SQ021) | 20 | 10.00% |
| Corporate volunteering eg awayday activity (SQ033) | 15 | 7.50% |
| Equipped play areas (SQ006) | 14 | 7.00% |
| Changing rooms or facilities for sports or other strenuous activity (SQ008) | 14 | 7.00% |
| Others, please specify below (SQ038) | 14 | 7.00% |
| Care for animals inc beekeeping (SQ016) | 11 | 5.50% |
| Foraging eg for mushrooms or wood (SQ027) | 11 | 5.50% |
| Performing arts rehearsal or performance (SQ030) | 11 | 5.50% |
| Organised sport (SQ034) | 9 | 4.50% |
| BBQ or other outdoor cookery (SQ031) | 8 | 4.00% |
| Informal competitive sport (SQ035) | 7 | 3.50% |
| Commercial food production (SQ014) | 5 | 2.50% |
| Outdoor medical consultations (SQ023) | 4 | 2.00% |
| Patients | n | Staff | n | Volunteers | n | Visitors | n | Local community or others | n |
|---|---|---|---|---|---|---|---|---|---|
| Walking (SQ002) | 128 | Walking (SQ002) | 155 | Walking (SQ002) | 74 | Walking (SQ002) | 117 | Walking (SQ002) | 100 |
| Informal gardening (SQ012) | 56 | Picnic areas (SQ016) | 72 | Informal gardening (SQ012) | 50 | Picnic areas (SQ016) | 52 | Cycling (SQ005) | 45 |
| Informal social (SQ027) | 49 | Active travel (SQ017) | 64 | Volunteering (SQ026) | 49 | Informal social (SQ027) | 47 | Running (SQ004) | 44 |
| Picnic areas (SQ016) | 42 | Informal social (SQ027) | 64 | Conservation tasks (SQ020) | 37 | Cycling (SQ005) | 35 | Picnic areas (SQ016) | 43 |
| Growing food (SQ013) | 40 | Cycling (SQ005) | 63 | Informal social (SQ027) | 36 | Wheeling (SQ003) | 32 | Informal social (SQ027) | 35 |
| Wheeling (SQ003) | 32 | Meetings (SQ019) | 45 | Growing food (SQ013) | 35 | Active travel (SQ017) | 29 | Informal gardening (SQ012) | 32 |
| Other exercise (SQ009) | 30 | Running (SQ004) | 44 | Picnic areas (SQ016) | 34 | Running (SQ004) | 26 | Other volunteering (SQ026) | 30 |
| Arts creativity (SQ022) | 29 | Informal gardening (SQ012) | 44 | Arts creativity (SQ022) | 29 | Informal play (SQ008) | 25 | Wheeling (SQ003) | 27 |
| Cycling (SQ005) | 24 | Other exercise (SQ009) | 32 | Active travel (SQ017) | 24 | Informal gardening (SQ012) | 21 | Informal play (SQ008) | 26 |
| Conservation tasks (SQ020) | 24 | Volunteering (SQ026) | 31 | Cycling (SQ005) | 19 | Volunteering (SQ026) | 21 | Birdwatching (SQ024) | 22 |
| Active travel (SQ017) | 22 | Changing facility (SQ010) | 29 | Other exercise (SQ009) | 19 | Other exercise (SQ009) | 18 | Other exercise (SQ009) | 21 |
| Birdwatching (SQ024) | 22 | Organised fitness (SQ011) | 28 | Meetings (SQ019) | 19 | Birdwatching (SQ024) | 16 | Active travel (SQ017) | 21 |
| Other Volunteering (SQ026) | 20 | Wheeling (SQ003) | 25 | Other nature study (SQ025) | 19 | Other nature study (SQ025) | 14 | Conservation tasks (SQ020) | 21 |
| Other nature study (SQ025) | 19 | Formal social (SQ028) | 20 | Running (SQ004) | 18 | Playground (SQ007) | 13 | Playground (SQ007) | 20 |
| Organised fitness (SQ011) | 17 | Growing food (SQ013) | 19 | Teaching (SQ015) | 18 | Arts creativity (SQ022) | 13 | Arts creativity (SQ022) | 20 |
| Informal play (SQ008) | 15 | Conservation tasks (SQ020) | 18 | Organised fitness (SQ011) | 16 | Meetings (SQ019) | 10 | Other nature study (SQ025) | 20 |
| Running (SQ004) | 13 | Birdwatching (SQ024) | 17 | Birdwatching (SQ024) | 16 | Foraging (SQ021) | 9 | Growing food (SQ013) | 18 |
| Meetings (SQ019) | 13 | Teaching (SQ015) | 12 | Formal social (SQ028) | 15 | Formal social (SQ028) | 8 | Organised fitness (SQ011) | 16 |
| Formal social (SQ028) | 13 | Medical uses (SQ018) | 11 | Wheeling (SQ003) | 14 | Other (SQ029) | 8 | Meetings (SQ019) | 16 |
| Medical uses (SQ018) | 10 | Arts creativity (SQ022) | 11 | Outdoor cookery (SQ023) | 12 | Organised fitness (SQ011) | 7 | Foraging (SQ021) | 12 |
| Outdoor cookery (SQ023) | 10 | Other nature study (SQ025) | 11 | Animal care (SQ014) | 11 | Growing food (SQ013) | 7 | Animal care (SQ014) | 11 |
| Teaching (SQ015) | 8 | Foraging (SQ021) | 6 | Foraging (SQ021) | 11 | Conservation tasks (SQ020) | 7 | Other (SQ029) | 10 |
| Foraging (SQ021) | 8 | Outdoor cookery (SQ023) | 6 | Informal play (SQ008) | 9 | Animal care (SQ014) | 6 | Competitive sport (SQ006) | 9 |
| Other (SQ029) | 8 | Competitive sport (SQ006) | 5 | Changing facility (SQ010) | 9 | Teaching (SQ015) | 5 | Teaching (SQ015) | 9 |
| Playground (SQ007) | 7 | Playground (SQ007) | 5 | Playground (SQ007) | 5 | Medical uses (SQ018) | 5 | Outdoor cookery (SQ023) | 9 |
| Animal care (SQ014) | 7 | Animal care (SQ014) | 5 | Medical uses (SQ018) | 3 | Outdoor cookery (SQ023) | 5 | Formal social (SQ028) | 9 |
| Changing facility (SQ010) | 5 | Informal play (SQ008) | 4 | Competitive sport (SQ006) | 1 | Changing facility (SQ010) | 4 | Changing facility (SQ010) | 4 |
| Competitive sport (SQ006) | 3 | Other (SQ029) | 2 | Other (SQ029) | 1 | Competitive sport (SQ006) | 3 | Medical uses (SQ018) | 3 |
| Answer | Medicine | Pathology | Clinical Oncology | Other cancer care | Imaging | Dental/Oral | Surgery eg orthopaedics | Obstetrics and gynaecology | Psychiatry |
|---|---|---|---|---|---|---|---|---|---|
| I do not know | 119 | 132 | 129 | 118 | 135 | 136 | 129 | 136 | 91 |
| No active use of the outdoor estate for therapeutic, medical or other service purposes to the best of my knowledge | 14 | 22 | 12 | 12 | 19 | 18 | 13 | 14 | 11 |
| Very limited active use of outdoor estate for therapeutic, medical or other service purposes to the best of my knowledge | 5 | 0 | 11 | 14 | 1 | 0 | 9 | 3 | 18 |
| Some active use of outdoor estate for therapeutic, medical or other service purposes to the best of my knowledge, including some use in treatment pathway plans and monitoring outcomes | 15 | 2 | 5 | 12 | 0 | 0 | 5 | 1 | 25 |
| Extensive active use of outdoor estate for therapeutic, medical or other service purposes to the best of my knowledge including active use or promotion in treatment pathway plans and active monitoring outcomes | 4 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 15 |
| Total number of answers | 157 | 158 | 158 | 157 | 156 | 155 | 157 | 155 | 160 |
| No answer | 43 | 42 | 42 | 43 | 44 | 45 | 43 | 45 | 40 |
| Answer | Occupational Health | Primary Care | Health Promotion | Clinical Support | General Acute, A&E | Estates | Facilities | Corporate | Other |
|---|---|---|---|---|---|---|---|---|---|
| I do not know | 107 | 104 | 82 | 131 | 133 | 116 | 119 | 114 | 73 |
| No active use of the outdoor estate for therapeutic, medical or other service purposes to the best of my knowledge | 12 | 14 | 11 | 11 | 17 | 9 | 12 | 16 | 3 |
| Very limited active use of outdoor estate for therapeutic, medical or other service purposes to the best of my knowledge | 9 | 17 | 17 | 3 | 1 | 9 | 8 | 10 | 1 |
| Some active use of outdoor estate for therapeutic, medical or other service purposes to the best of my knowledge, including some use in treatment pathway plans and monitoring outcomes | 22 | 15 | 30 | 6 | 1 | 12 | 8 | 8 | 2 |
| Extensive active use of outdoor estate for therapeutic, medical or other service purposes to the best of my knowledge including active use or promotion in treatment pathway plans and active monitoring outcomes | 6 | 7 | 17 | 2 | 1 | 6 | 4 | 3 | 1 |
| Total number of answers | 156 | 157 | 157 | 153 | 153 | 152 | 151 | 151 | 80 |
| No answer | 44 | 43 | 43 | 47 | 47 | 48 | 49 | 49 | 120 |
| Answer | LA | CHW | NA | CARTS | LG:HF | LG:SI | LG: CY | LG: EY | LG: CF | LG: O | Other |
|---|---|---|---|---|---|---|---|---|---|---|---|
| No knowledge (AO01) | 107 | 93 | 121 | 118 | 103 | 133 | 123 | 120 | 113 | 114 | 82 |
| Very limited involvement (AO02) | 22 | 18 | 6 | 11 | 15 | 10 | 13 | 17 | 11 | 17 | 2 |
| Some involvement (AO03) | 21 | 27 | 12 | 11 | 21 | 6 | 14 | 13 | 13 | 13 | 1 |
| Active involvement (AO04) | 5 | 10 | 6 | 10 | 13 | 3 | 3 | 3 | 8 | 7 | 3 |
| Active driver of activity (AO05) | 4 | 11 | 10 | 5 | 6 | 1 | 0 | 1 | 9 | 3 | 4 |
| No answer | 41 | 41 | 45 | 45 | 42 | 47 | 47 | 46 | 46 | 46 | 108 |
| Group | Abbreviation |
|---|---|
| Local Authority | LA |
| Charity: Health and Welfare Focus | CHW |
| National Agency eg Forestry Commission | NA |
| Conservation, Amenity or Recreation Charity or Trust | CARTS |
| Local Group: Health Focus | LG:HF |
| Local Group: Special Interest Focus (eg model engineering society) | LG:SI |
| Local Group: Children and Youth Groups | LG:CY |
| Local Group: Early Years | LG:EY |
| Local Group: Conservation focus | LG:CF |
| Local Group: other | LG:O |
The top involved organisations identified as being either actively involved or an active driver of activity were:
- Charities with a health and welfare focus (21/200 respondents).
- Local groups with a health focus (19/200 respondents).
- Local groups with a conservation focus (17/200 respondents).
- National agencies like Forestry Scotland (16/200 respondents).
- Conservation, Amenity and Recreation Trusts or Charities (15/200 respondents).
A surprising omission from this list, in view of some of the information from the earlier semi-structured interviews, are Local Authorities. However, if the response for ‘some involvement’ is included Local Authorities would occupy third equal position on the list with Local Groups with a Conservation Focus at 30/200 respondents each. On this basis the first two positions would still be occupied by Charities with a health and welfare focus, and local groups with a health focus respectively.
Property and Asset Management Strategies (PAMS) are the principal instrument by which the NHS estate is managed. Most respondents (66%) had not heard of PAMS, and another 19% had heard of them but had no idea of the extent to which they reflect health and well-being benefits (Table 5).
| Answer | Count | Percentage |
|---|---|---|
| I have never heard of PAMS (AO01) | 132 | 66% |
| Heard of PAMS but no idea of the extent to which they reflect health and well-being benefits (AO02) | 37 | 19% |
| Current PAMS do not reflect health and well-being benefits of the outdoor estate, potential or actual (AO03) | 3 | 2% |
| Current PAMS do not reflect health and well-being benefits of the outdoor estate but there are signs that future revisions will reflect these (AO04) | 8 | 4% |
| Current PAMS reflect the role or potential role of the outdoor estate but are vague or non-committal with regard to development and performance measurement (AO05) | 8 | 4% |
| Current PAMS have embraced the role of potential role of the outdoor estate, with analysis of existing contribution, clear objectives for future development or deployment and the adoption of performance measures which are regularly reviewed (AO06) | 4 | 2% |
| No answer | 8 | 4% |
| Totals | 200 | 100% |
The few remaining respondents divided almost equally around the division between the top and bottom two categories in the Likert scale we developed for this question.
Several of the survey questions invited additional comments and the survey attracted 204 additional comments in total. We have not conducted a formal thematic analysis of these comments, some of which were extensive, but the following themes easily emerge from them:
- Dog walking as a use was mentioned in response to several questions, with at least six references to this activity.
- Outdoor smoking was also mentioned, with three mentions of this activity one acknowledging its illicit nature in hospital grounds.
- Awareness of the potential benefits was clearly a broad theme for many respondents, while there were a smaller number of others who had never really considered that the NHS outdoor estate might be a therapeutic resource, captured neatly by one respondent who said, “Completing this survey has opened my eyes to the possibilities that the NHS outdoor space CAN be used for. It is something I had never thought about. I've always enjoyed walking around the grounds during my break and lunchtimes but never considered any other uses by other departments. I genuinely hope that the departments and/or wider agencies are encouraged to use the outdoor spaces in a more fruitful way”.
- Equally common was the recognition amongst respondents that much more could be done with the NHS outdoor estate through the implementation of practical adoption measures. This was coupled with a strong enthusiasm among respondents for more to be done.
- Pragmatically respondents also recognised difficulties in implementing good ideas for the greenspace, coupled with a sense of frustration at the demands on existing NHS resources. This frustration extended to the grounds management at some hospital sites, where it was recognised that management of greenspace could be more ambitious and imaginative in its engagement with the local environment and the needs of users.
- There was also an underlying sense of isolation amongst respondents, in that so many had so little idea of what was happening or could happen in areas of the NHS outside their own immediate experience and role.
Taken as a whole the survey shows:
- There is an extensive set of uses of the NHS Scotland estate – wider than is currently recognised in published sources.
- Walking is the dominant activity across all users. Future work could seek to distinguish different types and purposes of walking, distinguishing, for example, necessary travel to and from work; movement within the working day; and walking for other purposes including its own therapeutic or well-being impact.
- The top 10 uses identified by respondents to the survey were, in addition to walking: secure bicycle storage, active travel to and from work, picnic areas, informal recreational gardening, cycling, running, informal social gatherings, outdoor therapeutic interventions or rehabilitation and organised fitness sessions.
- Most respondents work in the NHS. There is scope to increase the external perspective on the use of the outdoor estate. More than three-quarters of the responses related to the following NHS Boards: Ayrshire and Arran, Tayside, Greater Glasgow and Clyde, Borders.
- In theory there is considerable scope to do a great deal more for therapeutic and well-being purposes with the NHS estate, and these benefits could be as strong for staff, visitors, volunteers, local communities as for patients. The results may even suggest that the benefits to the former groups could be at least as great or greater than for patients.
- There is a great enthusiasm for more extensive and better uses of the NHS Outdoor estate, but one obstacle to building on this asset will be the time and other resources required to do so.
- More formal promotion of the role of Property and Asset Management Strategies in the promotion of health and well-being uses of the outdoor estate could help to secure focus.
- Greater work to explore the inclusion of greenspace within formal health and treatment pathway protocols may also help to secure focus and commitment.
- The discussions beforehand, and to a lesser extent the survey, suggest that more could be achieved by working closely with non-NHS organisations in the development of new solutions on the NHS outdoor estate.
3. Assessing health and well-being benefits of the NHS outdoor estate – a conceptual model
This project has taken an integrated approach to the valuation of health and well-being benefits, a natural capital approach and a health economics perspective. Here, we use a natural capital approach to create a logic chain for the relationships between the natural capital assets of the NHS outdoor estate, the ecosystem services and benefits.
Natural Capital is defined as “..elements of nature that directly or indirectly produce value or benefits to people, including ecosystems, species, freshwater, land, minerals, the air and oceans, as well as natural processes and functions” (Natural Capital Committee, 2014). It is the stock of natural assets (e.g. soils, water, biodiversity) and supporting functions (soil formation, nutrient cycling) that produces a wide range of ecosystem services that benefit people. These include food production, regulation of flooding and climate, pollination of crops, and cultural benefits such as aesthetic value and recreational opportunities (Figure 2).
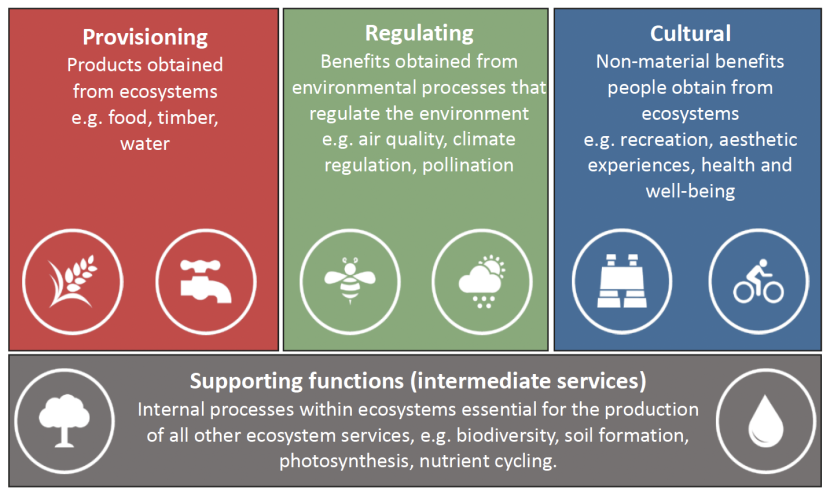
Figure 2. Key types of ecosystem services (Millennium Ecosystem Assessment, 2005). Note that supporting or intermediate services are now categorised as ecological functions (Haines-Young et al., 2018).
Click for a full description
They are the underpinning structures and processes that give rise to ecosystem services. Figure 2 is a diagram setting out the four key types of ecosystem services, namely provisioning services, regulating services, cultural services and supporting services. Provisioning services are products obtained from ecosystems such as food and timber. Regulating services are the benefits obtained from environmental processes that regulate the environment such as climate regulation. Cultural services are the non-material benefits people obtain from ecosystems such as health and well-being and supporting services are internal processes within ecosystems essential for the production of all other ecosystem services such as soil formation and photosynthesis.
As valuation is being considered in this project it is important to break down this concept further to ensure the environmental functions that lead to (physical) flows of goods and services (or benefits), and the economic production functions that lead to (monetary) flows of goods and services (or benefits) are considered separately. This splits the products of the natural system from the those of the social system and makes it clear which outputs require biophysical measurements and which outputs can be valued∗. As an example of this distinction, green health activities and water quality regulation are, respectively, final cultural and regulating ecosystem services, and stress reduction and clean drinking water are the health and well-being benefits that flow from these that can be quantified and valued.
3.1. Natural capital logic chain
One of the principal tasks of this project was to develop a conceptual model of the relationships between the natural capital assets of the NHS outdoor estate, and the health and well-being benefits that flow from them. A logic chain has been created (Figure 3) that describes the pathway that leads to a monetary value of those benefits. In addition, it includes the main factors that influence the delivery of health and well-being benefits from the NHS Scotland outdoor estate, as well as the beneficiary groups. Each stage needs to be measured to quantify the value.
The natural capital assets are the different habitats that may occur on NHS Scotland’s outdoor estates, e.g. woodland, gardens, allotments and grassland (Figure 3). These assets may alone give rise to final cultural ecosystem services such as recreation or restorative green health activities (e.g. walking, running, birdwatching), and certainly give rise to regulating services (e.g. air quality, noise and climate regulation). However, for many of the cultural services and the provisioning service of food production, further physical and social infrastructure will be required before the final ecosystem services and benefits can be realised. This might be the creation of cycle paths or footpaths and allotments, or organised activities such as exercise programmes (green gyms), conservation groups or therapeutic programmes. These all require labour and capital inputs. Whether or not the benefits are provided, or the extent to which the benefits can be provided, also depends on the accessibility of the greenspace provision (e.g. whether the natural capital asset is directly outside where a user is a patient or where they work, or is more than a few minutes away on foot or by bike, see Section 6 for discussion), how much greenspace there is available and the quality of the greenspace (whether it is well maintained or biodiverse).
The flow of health and well-being benefits are wide ranging (Figure 3), from stress reduction, increased mental health and happiness and sleep improvements, through lowering risk of chronic, metabolic and clinical diseases, to reducing pollution, noise, heat and flood hazards. This level of the flow of benefits is mediated by the exposure of beneficiaries to these greenspaces, whether any one visit is short or long, or whether these visits are daily, weekly or monthly. The benefits may increase if social interaction is also occurring during the visit/activity.
The logic chain (Figure 3) also outlines the beneficiaries of these benefits. In the NHS context these range from inpatients, outpatients, staff, and visitors and local communities, including individuals, families, school and nursery children. In relation to the cultural benefits these will flow directly to the users of the greenspaces. The regulating benefits will benefit those on site and those in surrounding communities. These benefits have value. Value can be captured in many ways, and we suggest an approach to evaluating and valuing these benefits in Section 5.
Any tool that is eventually developed for valuing the benefits that flow from the uses of the outdoor estate will also need to quantify the physical flows of these services. For provisioning and regulating services it is usual that the area and type of habitat is one of the determining factors that delivers a physical flow value (e.g. the area of woodland and species of tree will determine the amount of a pollutant adsorbed). It is more complicated for cultural services. The type, spatial location, accessibility, quality and quantity of greenspace will need to be measured as they certainly influence the type and frequency of activity that takes place, and hence the value. Ultimately the existence of greenspace determines whether there is a potential flow of these benefits or not. However, it is also necessary to quantify the number of people and their mental or physical response to being in the greenspaces, to complete the valuation. The Social Return On Investment framework proposed for use in the evaluation and valuation of health and well-being benefits (see Section 5 and 6) will pick up the full range of factors (environmental, social and economic) determining the value of the benefits whether or not they can be quantified. The importance of the natural capital assets will, therefore, be included. The type, location, accessibility, quantity and quality of the natural capital assets are even more important in a strategic context for the NHS Health Boards, as they determine how demand for these services can be met and where. Certainly, for organised activities like practical conservation and therapeutic gardening there needs to be the right amount of greenspace of the right type for the activity to go ahead. There can only be as many programmes as the space allows.
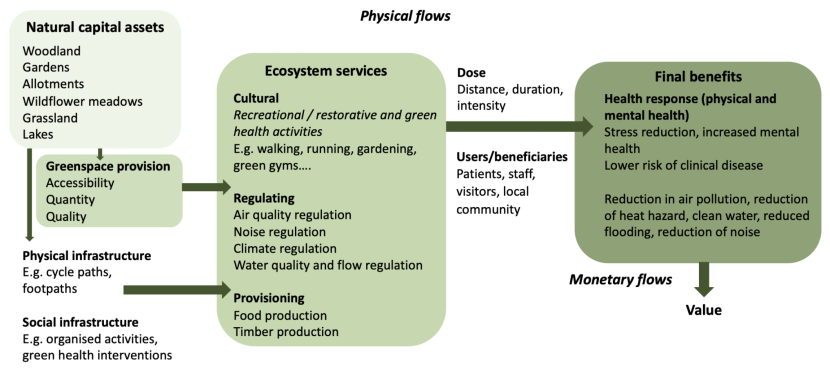
Figure 3. Natural capital logic chain outlining the relationships between natural capital assets, ecosystem services and health and well-being benefits on NHS Scotland outdoor estates.
Click for a full description
The above diagram shows the relationships between the natural capital assets (different greenspace types e.g. garden or woodland); the cultural ecosystem services such as recreation or restorative green health activities (e.g. walking, running, birdwatching), and provisioning and regulating services (e.g. air quality, noise and climate regulation) that give rise to health and well-being benefits (increased mental health and happiness, lowering risk of chronic diseases, including health benefits from reducing pollution, noise, heat and flood hazards). It also outlines the beneficiary groups (patients, visitors, staff and local community users) and emphasises that the health and well-being benefits and the regulating service benefits to these groups will vary depending on the type, spatial location, accessibility, quality and quantity of greenspace, the infrastructure that is provided (e.g. cycle paths, footpaths) and organised activities available (e.g. green gyms or practical conservation). All these elements need to be measured to enable a valuation of the natural capital benefits, i.e., the greenspace characteristics as well as the human use and benefits.
4. Valuing the health and well-being benefits of the NHS outdoor estate – rapid review and expert panel meeting
The aim of the rapid review was to identify scientific research papers and grey literature that contained metrics and toolkits for quantifying the health and well-being benefits (flowing from both regulating and cultural services) derived from activities in greenspaces related to the NHS outdoor estate. The focus was placed largely on the cultural services in the review, because there are fewer metrics available at present and it is a fast growing area of research. Regulating services that give rise to health and other benefits are better studied and there are already good metrics available.
Rapid evidence reviews are used in health sciences by Defra and in reviews commissioned by the Scottish Government. We drew on good practice from the Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews (Joanna Briggs Institute, 2017). The following questions guided the review:
- What are the health and well-being benefits from exposure to greenspaces of the type found on NHS estates? (Benefits delivered via provisioning, regulating services and cultural services.)
- What are the health and well-being benefits from specific health interventions (activities) employed by the NHS estates? (Benefits delivered via provisioning, regulating services and cultural services.)
- How are physical flow of benefits quantified? (Toolkits used or individual metrics.)
- How are the monetary values of these benefits quantified? (Toolkits used or individual metrics.)
The rapid review was focused specifically on papers and grey literature that quantify the relationships between the greenspace type (e.g. park / allotment / woodland) or intervention (e.g. green gym, therapeutic gardening) and the health and well-being response to exposure or participation (e.g. decrease in stress, increased quality of life, reduced mortality or morbidity). Web of Science and Google Scholar were searched to ensure that studies were captured from the scientific literature and the grey literature. The specific search terms used are outlined in Table 6 below. The search terms from the first two columns were combined with Boolean operators (e.g. “greenspace” AND “reduced morbidity”). Then a third search term from the third column was added (e.g. “greenspace” AND “reduced morbidity” AND “QALY”). Searches were also conducted using “green space” as well as “greenspace” to ensure all relevant studies were picked up. The searches were limited to research and grey literature published in the English language between 2000-2022. The scope outlined for this search was to keep the review concise and deliverable within the timeframe expected for a rapid review.
Relevant studies were first assessed by title and were taken from NatureScot and NHS Scotland reports supplied by the client. Key review studies that had been identified in the NHS Lothian natural capital assessment report were also included (62 studies, Figure 4). Two hundred and sixty-nine papers were accepted in this first stage of the review from the Web of Science and Google Scholar searches (Figure 4). Once these were screened for duplicates, irrelevant texts filtered out by reading the abstract, and excluding studies that were not accessible online, 165 studies met the inclusion criteria (Figure 4). A significant proportion (70%) of these papers were focused on quantifying the physical flows of the cultural and regulating services that deliver health and well-being benefits (e.g. measuring physical activity in greenspaces, morbidity or changes in physiological responses), and 30% were focused on valuing the health and well-being benefits.
| Greenspace type or activity | Response | Study type |
|---|---|---|
| Natural capital | Higher rates of physical activity | QALY |
| Greenspace | Recreational benefits | Cost benefit |
| Bluespace | Connection with nature | Cost-effectiveness |
| Natural environment | Social contact and cohesion | Case study |
| Urban green infrastructure | Mitigation of heat island effects Reduction of noise pollution | - |
| Parks | Reduction of air pollution | - |
| Gardens | Reduction of flooding | - |
| Allotments | Improved nutrition | - |
| Woodlands | Reduced mortality | - |
| Street trees | Reduced morbidity | - |
| Biodiversity | Better mental health | - |
| Green prescriptions | Better quality of life | - |
| Therapeutic gardening | Reduced health inequalities | - |
| Green gyms | Health interventions | - |
| Trails | - | - |
The papers accepted for full review were generally from natural capital, environmental economics, ecology, health economics and medical journals, with some reports from third sector organisations.
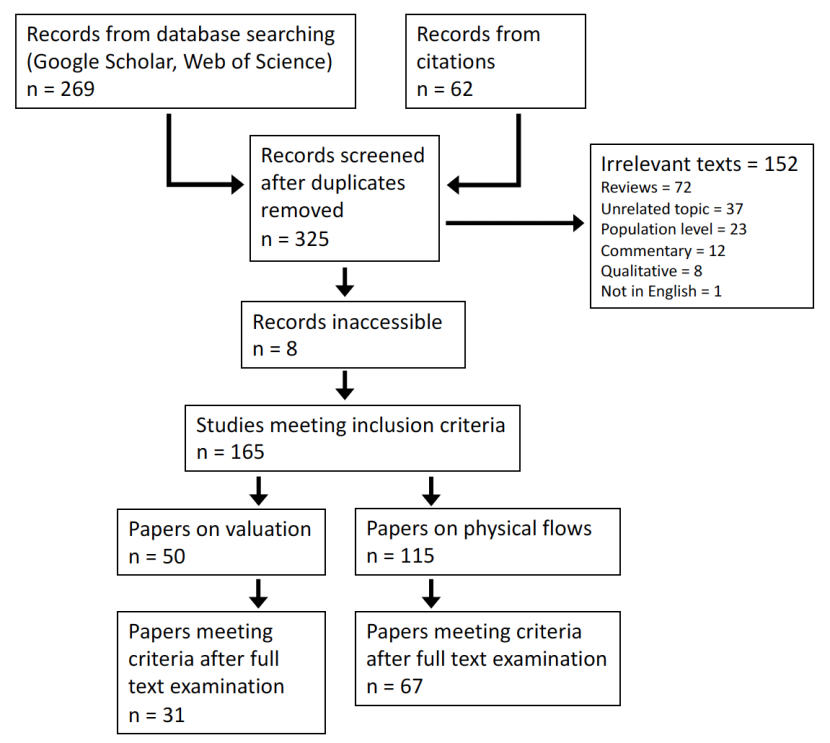
Figure 4. Flow diagram giving an overview of the rapid literature review concerned with metrics for quantifying and valuing the health benefits from the uses of greenspaces akin to those within the NHS Scotland outdoor estate.
Click for a full description
Figure 4 is a flow diagram giving an overview of the rapid literature review concerned with metrics for quantifying and valuing the health benefits from the uses of greenspaces akin to those within the NHS Scotland outdoor estate. Of the 325 papers found through citations and from literature databases, 152 were considered irrelevant and for 8 of the papers, records were not accessible. Of the remaining 165 papers, 50 focussed on valuation of natural capital and of this 50, 31 met the criteria for selection. 115 of the 165 papers focussed on physical flows of capital and of these, 67 met the criteria. In total, 98 papers met the selection criteria for inclusion in the literature review.
4.1. Physical flows literature
As mentioned above, a large number of the papers accepted for review were focused on the physical flows of the ecosystem services that give rise to health and well-being benefits. By this we mean studies that are quantifying the final ecosystem service, for example the green space activity (running, green gym or cycling) and the health and well-being benefit that is derived from that (e.g. stress reduction or reduction in morbidity). In order to be useful in the context of the NHS Scotland outdoor estate, it is important not only to record the metrics used to measure these, but also to note the type of greenspace from which these services and benefits were being delivered (e.g. allotment or woodland). This will enable an assessment of how appropriate these metrics are likely to be for the uses of the NHS outdoor estate that will be revealed by the survey.
Many of the physical flow studies focused on miscellaneous greenspaces, gardens or allotments, forests and urban greenspaces (Table 7). Fewer were associated with nature-based interventions, bluespaces, street trees, parks, trails and protected areas. A large proportion of the studies were concerned with the mental health benefits from activities in these greenspaces (Table 7).
| Greenspace type | No. studies | Final ecosystem services and benefits | No. studies |
|---|---|---|---|
| Misc. greenspace | 54 | Mental health | 56 |
| Garden/allotment | 23 | General health | 25 |
| Forests | 15 | Physical activity | 12 |
| Urban greenspace | 13 | Physical health | 9 |
| Nature-based intervention | 7 | Well-being | 9 |
| Bluespace | 3 | Mortality | 5 |
| Green exercise | 3 | Social cohesion | 3 |
| Street trees | 3 | Diet | 2 |
| Wetlands | 3 | Quality of life | 2 |
| Parks | 2 | Development | 1 |
| Trails | 2 | Morbidity | 1 |
| Protected areas | 1 | Recreation | 1 |
Metrics captured the final ecosystem services using occurrence, frequency of number of visits to greenspaces and these were related to specific types of activities, for example walking or allotment gardening. The benefits were measured in a variety of different ways depending on its nature. Studies concerned with mental health used questionnaires with related health scales specifically designed to quantify changes in different aspects of mental health. There were 49 different scales used, for example the Warwick Edinburgh Mental Well-being Scale, and the Perceived Stress Scale. There were also questionnaires and health scales to measure physical activity, for example the International Physical Activity Questionnaire and SQUASH. Studies were also concerned with measuring physiological responses from time spent in greenspace, for example heart rate, cortisol in saliva, blood pressure, that relate to reduction in stress responses.
Overall, these studies do find a positive link between activity in greenspace and an increase in health and well-being, but they are of mixed quality. The largest proportion of the studies focussed on general activities in greenspace, but the second largest on gardens or allotments. Some of the studies had very small sample sizes and often with no control. This means it is not possible to be sure whether the measured benefits are directly related to being in greenspace. An additional summary table has been created documenting the metrics used for quantifying the benefits associated with each greenspace type. It contains a score for quality and the reference of the paper or report. An excel spreadsheet also breaks this information down by study. These files will be made available to the project team.
4.2. Monetary flows literature
The monetary flows literature was focused specifically on valuing the benefits from activities or interventions set in greenspaces. There were a much smaller number (31) of studies focused on the monetary flow of the health and well-being benefits, than for the physical flows. There were a number of greenspace settings ranging from woodland to farms, and some studies focused specifically on benefits from cycle and footpaths (Table 8). Generally, the studies were focussed on specific interventions, for example ecotherapy which is a facilitated therapeutic intervention based in a natural setting, or green gyms which are supported sessions of outdoor conservation activities. The benefits in these studies were measured in terms of physical and mental health outcomes. Many of the papers were reviews of existing evidence that such interventions or activities can give rise to health and well-being benefits.
| Greenspace type | Intervention type or activity | Valuation methods for physical and mental health benefits |
|---|---|---|
| Woodlands and trees | Community Farm | Quality adjusted life year (QALY) |
| Urban woodland | Ecotherapy (e.g. Branching Out) | Disability adjusted life year (DALY) |
| Street trees | Green prescribing | Cost benefit analysis (CBA) |
| Protected areas | Recreational activity | Value of a statistical life (VOSL) |
| Farm | Gardening | Travel cost method (TCM) |
| Misc. green and blue spaces | Conservation | Contingent valuation (CVM) and Willingness to pay within this (WTP) |
| Community gardens | Walking | Health adjusted life year (HALY) |
| Cycle paths | Green gyms | Cost-effectiveness analysis (CEA) |
| Footpaths | - | Discrete choice experiment (DCE) |
| - | - | Social Return on Investment (SROI) |
A range of methods have been used in these studies, for example a focus on a change in hospital visits as a result of the activity or intervention, avoided deaths, changes in quality of life, morbidity or mortality, to enable a monetary value to be attached to the benefits (these metrics are listed in Table 8). Each valuation method takes a slightly different approach to quantifying and valuing the health and well-being benefit, and they are not mutually exclusive, e.g. it is possible to use QALY to measure health benefits within a cost-effectiveness analysis, and the monetary value of one QALY can be set by a Willingness to Pay analysis.
The QALY is commonly used in the environmental economics literature on its own and in the health economics literature within a Cost Utility Analysis. It is perhaps viewed as the gold standard because it is based on a standardised measure of health related quality of life in the form of a simple generic questionnaire (EQ-5D) that can be used at the population level in clinical and economic appraisal. A monetary value of one QALY can then be assigned to estimate the overall value of an intervention. In some cases, it is possible to translate health benefits already measured into the EQ-5D scale for QALY use (Hinde et al., 2021). However, rather than attempting to translate survey results into the QALY framework, other metrics as outlined in Table 8 above, that allow a monetary value estimate should be acceptable for use in the context of the NHS Scotland’s outdoor estate.
Overall, the rapid review demonstrated that there are relatively few studies that have tackled valuing the health and well-being benefits of activities in greenspace. The studies employ a wide range of methods for estimating the economic value of non-market goods and services ranging from the Travel Cost Method (TCM), Contingent Valuation (CVM) and Willingness to Pay (WTP) to QALYs, DALYs and Social Return On Investment (SROI). This suggests that a broad range of valuation methods are applicable, and some of them can be used together. The SROIs were generally found in the grey literature, rather than in environmental economics or health economics literature. The studies did not predominate from a particular country, studies cut across the UK, other European countries as well as Australia and New Zealand, so there does not appear to be an established best practice approach emerging in the scientific literature from a particular country. As with the physical flows literature, an additional summary table has been created documenting the metrics used for valuing the benefits associated with each greenspace type (see Appendix A2). It contains a score for quality and the reference of the paper or report. An excel spreadsheet also breaks this information down by study. These files will be made available to the project team.
4.3. Natural capital toolkits
Alongside the more formal rapid evidence assessment, a review of natural capital toolkits was undertaken. Natural capital toolkits bring together a range of metrics that can describe or quantify a broad suite of ecosystem service benefits. The toolkits range from those devised for general use, across any geographical location but at a landscape scale (e.g. InVEST), to those created specifically for use at smaller scales and in relation to e.g. urban developments (originally the aim of the NATURE tool). Some of the toolkits are spatial so use GIS mapping, some are spreadsheet based. A number of the toolkits are focused only on the physical flow of benefits (e.g. EcoServ R) and do not include the valuation step. Some of these toolkits, although including cultural services, are qualitative measures (e.g. NATURE tool and the Environmental Benefits of Nature Tool). The focus here is on tools that can be used to quantify and value health and well-being benefits. A list of the most appropriate tools are listed in Table 9.
| Natural capital toolkits |
|---|
| Health Economic Assessment Tool (HEAT) |
| Environment Valuation Online (NEVO) |
| Outdoor Recreation Valuation (ORVal) |
| Integrated Valuation of Ecosystem Services and Trade-Offs (InVEST) |
| iTree Eco |
| Green Infrastructure Valuation Toolkit (GI-Val) |
| Co$ting Nature |
| Benefits Estimation Tool (B£ST) |
| Greenkeeper |
Reviewing the natural capital toolkits (Table 10) showed that no one tool would be suitable for use in measuring the health and well-being benefits across the NHS Scotland’s outdoor estate. Certain elements of each of the tools may be useful in particular circumstances. The World Health Organisation’s HEAT tool is focused on the benefits of cycling and walking only, and the valuation is based on the reduced risk of walking where there is no traffic. This may have some use if NHS greenspaces are being used as alternative routes by recreational walkers or commuters.
The NEVO tool created by the University of Exeter maps and values a number of ecosystem service benefits (agricultural production, timber production, carbon sequestration and recreation). The recreation valuation in this tool uses a model derived from the ORVal tool, also created by the University of Exeter. The ORVal tool uses a statistical model called a Recreational Demand Model to predict the number of visits that are made to currently accessible greenspaces by adult residents of England. The number of visits are modelled using data from the Monitor of Engagement with the Natural Environment (MENE) survey, and adjusted based on factors such as socioeconomic characteristics of people, the day of the week, attributes of the greenspace, the availability and quality of any alternative greenspaces. The model, through a welfare function, also describes the welfare an individual derives from making different recreational choices, and the welfare values are, therefore, provided by the tool. The welfare gained from a particular greenspace will depend on a number of factors (e.g. socio-economic status, month of the year) and the benefits experienced at a site is traded- off against the costs of travelling to the site. These tools are unfortunately focused only on England. However, the metrics used for the suite of services they cover are transferable, and some could be useful in a tool focused on NHS Scotland’s outdoor estate.
InVEST is a suite of models used to map and value the benefits from nature, created by the Stanford University Natural Capital Project. The models include 17 different ecosystem services. These models are for use at the landscape scale, so would not be suitable for this context. There are models, such as urban cooling, urban flood risk mitigation, recreation and scenic quality that may contain metrics that could be transferred for use in this project.
iTree eco is a toolkit developed by the United States Forest Service that can be used in the UK. Based on data on woodland and individual trees it can quantify and value pollution removal and human health impacts, carbon sequestration and storage, and avoided run-off, interception and transpiration. These are useful models that can be applied to woodland and tree habitats of the outdoor estates.
GI-Val is a toolkit devised by the Mersey Forest in England. It is a set of spreadsheet tools that can quantify 11 different benefits that might flow from green infrastructure. These include recreation and health and well-being. However, the quantification and monetisation of the health and well-being services in this tool require further research. The tools are a mix of metrics and monetary values transferred from case studies or other toolkits. The toolkit is suitable for application at the estate scale as it has been designed to assess specific green infrastructure interventions. Some of the metrics could be useful for an NHS outdoor estate/urban natural capital toolkit.
Co$ting Nature is a spatial policy-support tool for natural capital assessment and accounting, developed by Kings College London, AmbioTEK and UNEP-WCMC. It maps 18 different ecosystem services and can combine these with maps of conservation priority. The focus is on the opportunity cost of protecting nature to produce ecosystem services, rather than valuing nature (although it does have some valuation models within it). It is useful for assessing the impacts on ecosystem services of human interventions for conservation prioritisation and planning. This is likely to work best at large scales, and due to this the resolution is unlikely to be appropriate for use in this context.
The B£ST created by Stantec and EcoFutures is a spreadsheet tool that provides guidance to estimate the monetary benefits of Blue Green Infrastructure, including Sustainable Drainage Systems and Natural Flood Management. It is able to quantify and value 14 different service benefits. It does not include health and well-being benefits. It is designed for use at small scales and there may be metrics that can be extracted from here and used in this project.
Greenkeeper is a spatial tool created by Vivid Economics, Barton Willmore and the University of Exeter to quantify and value the health and well-being and carbon sequestration benefits that flow from urban greenspaces in the UK. The tool uses a random utility recreational demand model (similar to ORVal) which estimates recreational visits to urban greenspaces. It uses these visit numbers and applies a series of valuation methods to estimate the monetary value of physical health and mental well-being benefits at the individual and local population level. It is the only existing toolkit that focuses on monetising the health and well-being benefits from urban greenspaces. Whilst it would be very applicable for use on the NHS Scotland estates, it is proprietary, so the exact methodologies used are not available. It is, therefore, difficult to assess the quality of this tool.
The review of the natural capital toolkits revealed a range of different metrics associated with health and well-being benefits. No one toolkit will be useful for developing a tool for measuring the benefits from the outdoor estate, but specific models or approaches within them may be appropriate for certain uses of the estate.
4.4. Expert consultation
An expert panel meeting was held on the 8th March 2023 via Teams. It brought together three leading experts in the field of Health Economics, Prof. Rhiannon Tudor Edwards founding Director of the Centre for Health Economics and Medicines Evaluation (CHEME) at Bangor University, Prof. Mary Lynch from the School of Health and Life Sciences at the University of the West of Scotland, and Prof. Emma McIntosh from the School of Health and Well-being at the University of Glasgow.
The aim of the expert panel meeting was to discuss the appropriateness and robustness of the methods and approaches to valuing the health and well-being benefits associated with the NHS outdoor estate identified in the review. Importantly, it was also to find out their recommendations on how to best approach the valuation of these benefits, what the aspirations for this challenge should be, and the data required to fulfil the project aim. The programme for the discussions is in Appendix 3 and outlines the specific questions devised to direct the conversation. However, from the beginning the academics had quite clear ideas as to what would be required to achieve the ultimate goal of valuing the health and well-being benefits of the NHS Scotland outdoor estate, and so the conversation evolved from these.
Time was spent discussing the key concepts on which any framework for valuation of the health and well-being benefits would need to be based. For example, those related to delivering prevention of chronic health conditions and health inequalities such as anchor organisations and the place-based approach. Discussions were also focused on the need to use methods that allow both qualitative and quantitative valuation of the benefits; recognising there will be different views of greenspaces, their use and value; viewing the green and bluespaces as natural experiments, and understanding that social and economic factors will impact on the success of green health interventions. The type of framework that could deliver this was then laid out, the merits of using a modular approach nesting frameworks like Cost Consequence Analysis with Social Return on Investment, and delivering a way of appraising options across all priorities in estate scale business plans. The discussion then turned to how the framework could be applied, the data that it would be necessary to collect on the natural capital assets, the quality and accessibility, use and benefits; the variety of greenspace uses by different groups, and ways of promoting greenspace use. The academics then advised on the areas to focus on in the short term that might have the most impact, e.g. a focus on the health and well-being benefits of NHS Scotland staff, and mental health across all users, and ideas for valuing benefits in the medium and long term.
The meeting was an excellent discussion. The academics were keen to highlight that what this project is attempting to do is cutting edge, and that tackling the challenge requires a broadening of the tools and techniques used by Health Economists. The following two chapters and the recommendations are based directly on the discussions.
5. A framework for evaluating and valuing the health and well-being benefits of the NHS Scotland outdoor estate
Here we outline what we are calling a “building blocks” framework that will allow both the evaluation and the valuation of health and well-being benefits flowing from the NHS Scotland outdoor estate. The framework provides a pathway towards a robust assessment of the benefits, ensuring that these benefits are considered fairly alongside other priorities (e.g. the delivery of new hospital buildings) in NHS estate business cases. It recognises the need to address how the outdoor estate is viewed now, and importantly is built on aspirations for the role the outdoor estate can play for staff, patients and the local community in the short, medium and long terms, aligning with the priorities outlined in the NHS Scotland Climate Emergency & Sustainability Strategy. Before we describe the framework itself, we explain its theoretical and conceptual underpinning. It is worth pausing here to note the importance of time-horizons in public health and preventative interventions. Many benefits to physical and mental health and the life-time health opportunity architecture of the population involve costs now and benefits many years in the future. It is worth using a building blocks approach to capture short term metrics such as footfall and qualitative responses by staff to, for example, zoning of staff amenities outdoors and changes to work culture to enable use of that greenspace, and longer term benefits to be captured e.g. through social return on investment methods. These may relate to increased use of the NHS green estate by local communities enhancing urban neighbourhoods and preventing antisocial behaviour, encouraging urban food production, shared space for walking and cycling, outdoor gyms, and other uses. Long term benefits may include less demands on primary care services through avoided mental health and physical health problems that relate directly to increased physical activity, improved social networks, and joined-up development at a neighbourhood level which incorporates use of the NHS green estate.
5.1. Conceptual background
A place-based analysis
The framework is place-based in accordance with guidance in the HM Treasury Green Book (Annex 2) (H.M. Treasury, 2022). This means that it takes account of the issues, interconnections and relationships in a place, and coordinates action and investment to improve the quality of life for that community (community in this case can be patients, staff and those living in neighbourhoods in the proximity of estate sites). We know the importance of neighbourhoods as a way of explaining socioeconomic gradients in quality- adjusted life expectancy (Marmot, 2020). The physical location of estate sites within the urban-rural context needs to be factored into assessments of value. When considering the benefits to the wider community of NHS estate greenspaces, they are likely to be of higher value if they are located in lower socio- economic areas such as inner cities or deprived rural areas. We recognise that poverty exists in urban settings and rural settings and that they are materially different. Perhaps the argument here is that in built up areas where there is a lack of accessible green space, a new offer of access to NHS estate greenspace could provide a marginal benefit of value. Green space in rural areas is often less of a problem than access to e.g. public transport, activities, shops and other facilities.
The place-based concept also links to the idea of NHS estates as anchor organisations. As an anchor organisation there is a need for the significant land and physical assets of NHS Scotland to contribute a positive influence on the social, economic and environmental factors that help create good health within local neighbourhoods, playing a key role in addressing health inequalities (Reed et al., 2019). Many of these inequalities relate to differentials in life-time health opportunity architecture across ethnic minority groups (Cronin-de-Chavez et al., 2019). Much was learnt during the COVID-19 pandemic about this differential (Cheshmehzangi, 2022). NHS Scotland as an anchor organisation is a specific focus of the Place and Well-being programme within the Scottish Government’s Care and Well-Being Portfolio (Scottish Government, 2022b), and links to the Public Health Scotland Place and Well- being Outcomes (Public Health Scotland, 2022). This role as anchor organisation is also recognised within the NHS Scotland Climate Emergency & Sustainability Strategy (Scottish Government, 2022a) as an opportunity to model the sustainability goals around net- zero carbon, fair employment, gender equality and sustainable communities to ultimately tackle inequalities. Viewing the NHS as an important contributor to socio-economic and environmental improvement is also already reflected in the Public Procurement Act 2016 in Scotland (Scottish Government, 2016). This requires that procurement achieves wider social benefits, for example promoting community benefit and compliance with equality duties, economic benefits, for example ensuring support of SMEs and third sector, and a contribution to Scotland’s climate change targets.
As part of this place-based approach the NHS Scotland outdoor estate should also be key in delivering health and well-being benefits to its own workforce, thereby supporting the recruitment, retention and resilience of the workforce. Absenteeism is a key challenge in the NHS (NHS Education for Scotland, 2022), and ensuring access to quality greenspace on site for use during breaks, after shifts and in leisure time is important. Providing access in itself is not enough. Allowing staff to have the time for breaks outside in the greenspace is critical. This will require influencing the working culture in NHS Scotland healthcare sites.
The place-based approach and the philosophy of the anchor institution is based on reducing health inequalities with a focus on neighbourhoods and communities rather than individuals. This requires an understanding of the complexities of context and causes of these inequalities which will not be addressed if the NHS operates solely as a downstream organisation treating acute illness when it arises. There needs to be a shift in focus to illness prevention and the concept of well-becoming across the life-course (Edwards et al., 2019; Edwards, 2022). Considering the estate as more than the sum of its buildings (grey infrastructure) but as a whole estate with important green and bluespaces is central to the prevention of illness for the whole community. Figure 5 shows the NHS Scotland hospital green space estate as a future upstream contributor to prevention of ill-health and disability. This would require a broadening of perspectives at every level (government, NHS decision makers, medical staff), and is key to being able to integrate the value of health and well-being benefits of the NHS Scotland’s outdoor estate and begin to fully apply the proposed framework.

Figure 5. Moving upstream – the NHS Scotland hospital green space estate as a contribution to prevention. NHS Scotland is currently positioned downstream of the challenges causing chronic health conditions and health inequalities.
Click for a full description
Figure 5 is a graphic contrasting a hospital with lots of surrounding greenspace with a hospital where the surroundings are mostly hard-standing areas or ‘grey-infrastructure’. It demonstrates that hospital estate is more than the sum of its buildings but should be thought of as a whole estate with important green and blue spaces that are central to the prevention of illness for the whole community.
The proposed framework has been designed specifically to capture qualitative and quantitative valuation of the health and well-being benefits of the NHS outdoor estate. Well-being benefits are notoriously challenging to capture because of the difficulties in quantifying the benefits and estimating non-market values. Consequently, it won’t be possible to estimate a monetary value for all health and well-being benefits, but the framework allows other types of (non-monetary) valuation to be captured for consideration in decision-making. Recognising this requires a reframing of the level of evidence required for valuation, an understanding that it will not be possible to complete randomised controlled trials within this context, so what is viewed to be the ultimate in robust evidence is not attainable. It is important to view the use of green and bluespaces that make up the outdoor estate as natural experiments, and to employ an evaluation process that captures monetary and non- monetary valuation.
Realist evaluation approach
A realist evaluation underpins this framework. Realist evaluation is based on the assumption that a specific intervention will not work in every context and for all beneficiaries. This approach focuses on the nuances of the impacts of the intervention, for example “what works, for whom under what circumstances and how” (Wong et al., 2016; Mercer et al., 2021). This recognises that social and economic systems are integrated and that factors such as culture, class and type of economic systems have a real effect on whether programmes work. This approach is used for evaluating complex interventions, such as green health interventions we might be concerned with in the context of the NHS outdoor estate. The three key pillars of a realist evaluation are context, mechanisms and outcomes (CMO).
Widening evaluative space
Importantly, the proposed framework is also widening the evaluative space. That is, it recognises that there is pluralism in values and that these can be different and conflicting and that they are not reducible to each other or an ultimate value. In this context there are likely to be different views of greenspaces, their use and their value, and it should be recognised that delivering a monetary value is only one way of capturing this (see evaluation and valuation above). The proposed process is designed to capture a wider array of possible values. To achieve this it is important that there is staff, patient and public involvement in the process of this evaluation to ensure the important benefits are being captured and the range of values are being considered in the process.
Integrating natural capital accounting and health economics
The proposed framework integrates the natural capital accounting approach and a novel health economics approach to measuring health and well-being benefits from the natural environment (borrowing methods from environmental economics). As outlined in the logic chain of the relationships between the natural capital assets of the NHS estate (Figure 3, Section 3), the ecosystem services and benefits, some health and well-being benefits are derived from the provisioning and regulating services (e.g. local food production and air quality regulation), but the health benefits from the cultural services (e.g. recreation) will be more numerous and significant. Step 2 of the framework (Section 5.2 below) will identify benefits that are derived from all of these categories, and appropriate methodologies can be applied. Environmental benefits that are not delivered as direct health and well- being benefits, for example, carbon sequestration, can also be identified at this point and dealt with using established natural capital valuation methods.
5.2. The framework
The proposed evaluation and valuation framework is an integrated and modular approach (see Figure 6). This figure sets out three building blocks sitting on a “place-based” approach taking a number of time-horizons into account. Along the right hand side we list a number of key considerations relating to stakeholders, methods, perspectives and focus. On the left we summarise the task which involves identification, measurement, valuation of both costs and outcomes of the use of the NHS outdoor estate to support health and well-being. The first step uses a cost consequence framework that captures costs and impacts associated with the outdoor estate activities and interventions (Figure 6). This aligns with guidance from the National Institute for Health and Care Excellence (NICE) (NICE, 2011 and 2012) for the evaluation of public health interventions which emphasises the appropriateness of cost consequence and cost benefit analysis, taking a wider intersectoral perspective on the identification, measurement and valuation of costs and benefits. The second step uses a social cost benefit, Social Return On Investment (SROI) framework, centred on the NHS outdoor estate, for evaluating and valuing the benefits associated with it, using the Treasury Green Book as a benchmark. The third step is concerned with the prioritisation of competing demands at the whole estate level using multi-criteria decision analysis, for the assessment of competing demands on NHS estates.
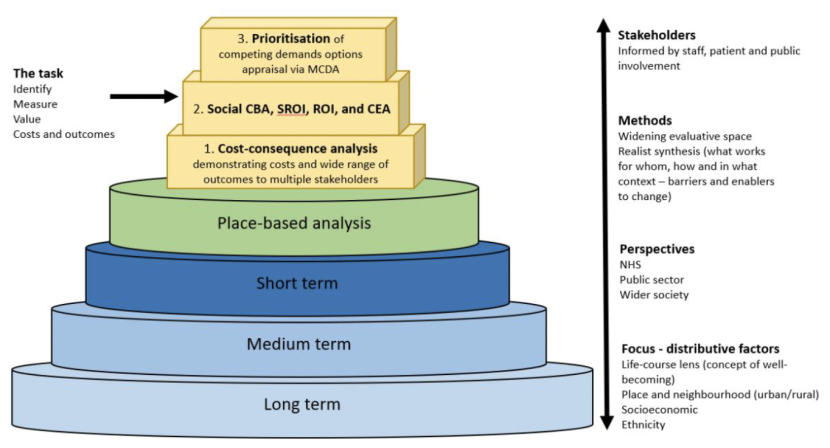
Figure 6. Framework for identifying, measuring and valuing the health and well-being benefits of the NHS Scotland outdoor estate within with a wider context of prevention policy.
Click for a full description
Figure 6 shows a series of building blocks that are needed in order to evaluate the benefits from the NHS outdoor estate. The blocks become smaller up a y axis with each block slightly smaller than the one beneath, forming a pyramid. The bottom three blocks are labelled Long Term, Medium Term and Short Term respectively, indicating the importance of different time perspectives on how you evaluate the NHS estate. The forth block in the series is labelled Place-based analysis. The next three blocks are concerned with analysis of the stakeholders involved, the outcomes for those stakeholders, the valuation of those outcomes and the prioritisation of different demands from stakeholders.
Cost consequence analysis (CCA) is a form of economic evaluation where disaggregated costs and a range of outcomes are listed to allow the decision-makers to decide on their relevance and relative importance (National Institute for Health Research, 2018). Within the National Institute for Health and Care Excellence (NICE) framework, decisions on whether or not to fund interventions are based on incremental cost-effectiveness analysis using a standardised quality adjusted life year (QALY) (NICE, 2012). However, the outcomes from green health interventions or general recreational activities in the NHS outdoor estate do not fit neatly into this conventional economic evaluation framework, because there will be multiple and varied outcomes (both health and non-health) associated with them. For example, whether a greenspace is used or not, or how it is used and how often, will be influenced by socio-economic background, the location of the estate site, accessibility of the site, its quality and other health and lifestyle factors of the user/beneficiary. CCA allows the consideration of broader outcomes of these interventions and activities, hence broadening the economic evaluative space (Willings, 2017), which is considered important in relation to public health interventions.
The advantages of using this approach in step 1 of the framework, and in the context of the health and well-being benefits associated with the NHS Scotland outdoor estate, are that it:
- Allows a summary of a broad range of costs and benefits (outcomes) of the activities on the NHS outdoor estates, those that are associated with health and non-health outcomes. It provides a broader and richer source of economic information that will be needed in Step 3 of the proposed framework.
- Can include the whole range of activities, whether or not they have been valued.
- It is an approach that can be easily understood and applied by decision-makers.
- This process recognises that the activities associated with the NHS outdoor estate are complex interventions (Skivington et al., 2021) and can identify this complexity. It will allow suitable economic methods to be refined to capture this complexity for a more robust evaluation and valuation of the benefits.
Step 2. Social Return on Investment
The next step of the evaluative process is to apply a Social Return on Investment (SROI) framework to assessing the activities/interventions in the NHS outdoor estate listed in the CCA (Step 1), at the same time as applying a mixed methods approach to valuation ensuring that the right methodology is used to value the right activity. The focus of the SROI would be the NHS outdoor estate itself (as opposed to an organisation or specific intervention). The SROI framework is specifically designed for measuring and accounting for a broader concept of value (Nicholls et al., 2012). It aims to promote human well-being at the same time as reducing inequity and environmental degradation. It does this by incorporating social and environmental costs and benefits in addition to the economic ones. This allows an understanding of the complexity of the intervention, the plurality of values, and uses monetary value to represent the outcomes. A cost benefit ratio is estimated, indicating the amount of benefit or social value (£) delivered for every £1 invested. SROI can be undertaken retrospectively or be used to predict the social value delivered in future scenarios.
The benefit of using this framework is to ensure that the full complexity of the value of the benefits or impacts is captured. The intention is that the appropriate methodology will be chosen for the activity in question. These are likely to be Stated Preference methods such as the Contingent Valuation Method (CVM), which includes Willingness to Pay or Willingness to Accept (WTP/WTA), or Choice Experiments. The Travel Cost Method may also be appropriate for measuring recreational benefits, and can be integrated with CVM. We will talk more about valuation methods and data required for use of these techniques in Section 6 below.
The benchmark for this step will be the Supplementary Green Book Guidance “Well-being Guidance for Appraisal”39. This lays out the stages for a robust evaluation and valuation of health and well-being benefits from cultural services, using Social Cost Benefit Analysis (Social CBA) which is akin to the SROI framework (Edwards et al., 2021; Fujiwara, 2014; Fujiwara, 2015; Hutchinson et al., 2019; New Economics Foundation Consulting, 2020; Nicholls et al., 2009). It presents principles for measuring, quantifying and monetising well-being as well as for monitoring and evaluation.
Similarly for the valuation of the provisioning and regulating services that give rise to health and well- being benefits as part of this step, appropriate methods can also be derived from the Green Book, but additionally the Defra ‘Enabling a Natural Capital Approach’, which appraises valuation methods across a range of provisioning and regulating (and cultural) ecosystem services (and contains the most commonly used methods (DEFRA, 2020). Whilst the Defra ENCA guidance does cover valuation methods for cultural services, we are not suggesting it is used in this context. This project is proposing a more nuanced and robust assessment of cultural services than provided in the ENCA guidance, and we are therefore suggesting that this is used only for the provisioning and regulating services.
Step 3. Prioritisation – options appraisal
Any framework for evaluating and valuing the health and well-being benefits from the NHS outdoor estate would not be complete unless it can feed into an options appraisal. It is clear from the conversations with NHS professionals engaged in improving public health, as part of this project, that the desire for the health and well-being benefits to be valued is driven by the need for these to be balanced against other priorities at the estate scale, for example, increasing grey assets within the estate, or options for the design of new hospital sites, that are more easily valued in a cost benefit analysis within a business plan.
We suggest multi-criteria decision analysis (MCDA) as a final step for the assessment of options across the NHS estate. It supports decisions makers that are faced with evaluating multiple conflicting alternatives and provides a way of combining them in one overall appraisal (Oliveira et al., 2019). MCDA provides a toolbox of concepts, models and tools and is a clear framework for making decisions about conflicting priorities and the most efficient allocation of resources (i.e. is appropriate when budgets are fixed). MCDA typically consists of the following phases: problem identification and structuring, model building and use, and the development of action plans (Thokala, 2011). MCDA modelling has four stages:
- Identifying the alternatives to be appraised.
- Identifying the criteria against which the alternatives are to be appraised.
- Scoring of the value of an alternative’s expected performance against the set criteria.
- Criteria weighting – reflecting which criteria are considered a priority over others.
The first two phases are problem structuring, which involves meeting all relevant stakeholders. After this there are a number of different mathematical models that can be used in MCDA that will aid the comparison of options, for example, (i) value measurement models that measure the degree to which one decision option is preferred to another by creating and comparing numerical scores, (ii) outranking models that is a pair wise comparison of criterion and (iii) goal, aspiration or reference level models that derive alternatives which are the closest to achieving the pre-set criterion in the most satisfactory way.
The advantages of using MCDA are:
- It is able to account for stakeholder preferences and values.
- It provides a transparent reporting format.
- It could aid the understanding of multiple values and data gaps.
- Highlights the difference between evidence and value judgement.
- Clear outputs that are easily understandable.
- Robust and accountable.
Practical considerations are that decision makers may need training in MCDA techniques and any specialist software required, although it is possible to employ facilitators and experts to aid the process.
6. Practical application of the framework
It is important to recognise there are many other variables that need to be measured before it is possible to assess the full complexity of the value of the benefits (derived from the natural capital assets, cultural, regulating and provisioning services, see logic chain Figure 3, Section 3) and impacts of green health interventions from use of the NHS Scotland’s outdoor estate. These are the type, amount and quality of the green and bluespaces, how the space is being used (activity types), by whom and how often, and what are the benefits they are receiving. Here, we outline the requirements for putting the proposed framework into action (using the headings from the logic chain in Figure 3), but then offer a way forward for NHS Scotland to begin to evaluate and value the benefits from the outdoor greenspace now, and what actions will be required to achieve this in the medium and long term.
6.1. Data
Natural capital assets, quality and accessibility
Valuation of the benefits associated with the NHS outdoor estates is only possible if there is data on the green and bluespaces within it. Public Health Scotland are developing a Geographic Information Systems (GIS) map of the NHS outdoor estate in Scotland that spans the 14 territorial Health Boards, 7 special Health Boards and 1 public health agency. The intention is that the GIS map will include a typology of habitats, but also the quality of the habitat for biodiversity (Holt et al., 2021). This is key information for creating a biodiversity and ecosystem services provision baseline. This exercise is important not only in natural capital terms, but also as an audit of the estate’s green and bluespaces. Some boards may not already have a list or a map of all of the estate sites they own, let alone a map of the greenspaces within them. The GIS mapping will not only give the Scottish Health Boards an understanding of the spatial location of their outdoor estate, inform the development of NHS Board Open or Greenspace Strategies, but can also be used to put the NHS estates in a broader community and local authority context. The maps can be used to understand the proximity of greenspaces entry points to local communities and relate other social data to this, for example indices of deprivation, census data and ascertain which communities are within 10 mins on foot or by bike from estate spaces (Scottish Government’s 20-Minute Neighbourhood Plan (Scottish Government, 2022c)). It can also be used to understand how the outdoor estate links to other greenspaces within the Local Authority region, identifying nature and active travel networks and allowing alignment with Local Authority Open Space Strategies.
Whist quality related to biodiversity has been shown to increase health and well-being benefits (Dawkins, 2022), the quality of the greenspaces can also be captured in terms of how usable the space is for recreational activity or green health interventions. There are studies that suggest that the more natural the greenspace, the more beneficial it is for human health and well-being, for example a woodland would offer higher health and well-being benefits compared to amenity grassland. Litter or graffiti may be a problem and greenspaces near woodlands may be perceived as unsafe. This will all impact on the way the beneficiary groups do or do not access and use the outdoor estate.
At this stage it is also important to consider assessing the accessibility of the greenspaces to the different user groups. This is understanding supply in relation to demand both by physical location, but also considering the social and economic reasons that may make sites inaccessible (e.g. transport, poverty, or simply not knowing that the sites are there and can be used, or wider considerations of safety or perceptions of safety, e.g. not having lit spaces for breaks for those that work night shifts on site).
Understanding the quality and accessibility can also ensure that the physical infrastructure that allows use suited to the beneficiaries can be delivered. Beneficiaries will have different needs, and there will be additional requirements for hospital patients with particular conditions, those with physical and learning disabilities and sensory impairment (Greenspace Scotland, 2022). Access and building design using social sustainability principles (as set out in the Sensory Trust’s Social Sustainability Toolkit), and creating sensory experiences e.g. gardens and trails (as set out in the Sensory Trust’s Gardens and Greenspace Guidance) will be key. Hospital sites are open 24 hours a day, seven days a week, therefore, greenspaces need to be accessible 24 hours a day. They need to ensure areas of access for staff breaks which may require privacy; access near to where patients are located, for example, sitting and appreciating nature, through sensory gardens or for therapeutic gardening; and meeting the needs of local communities by providing access to greenspace for walking/cycling or providing play areas. They need to provide safe places for all with lighting and weather proofing for use in all weathers. This should include planning for future pandemics where space allows patients to meet visitors outside, rather than visitors going into buildings, and for supporting an aging population who spend longer in the health care system. NHS estates also need to identify where they are providing accessible greenspaces for local inhabitants that are within a 10- minute walk or bike ride. However, it should not be assumed that simply providing the greenspace means that people will use it. Novel approaches will be required to encourage use of NHS estate sites for impacting health inequalities (Olsen et al., 2022). Data on users of the estate greenspaces could be gathered as part of an annual survey of well-being benefits related to greenspace (see recommendation below). Understanding the profile of people using the greenspaces now will aid the identification of those who are not accessing these spaces.
NHS estates will have to be carefully managed for the range of different uses and user groups. A zoning of the outdoor estate within larger sites could provide the following:
- Areas for staff only for use in breaks and after shifts.
- Areas that provide privacy for patients and their visitors.
- Greenspace areas that are close to patient accommodation.
- Areas for leisure.
- Accessible greenspace for the local community.
- Areas for special interest activities, for example practical skills development, environmental study (e.g. birdwatching) or community food growing.
Smaller sites might be selected for particular uses and user groups with a strategic plan for how these are spatially allocated.
Ecosystem services - use
Capturing the final ecosystem services requires data on how the site is being used (e.g. gardening, walking, green gym, outdoor therapy programmes, bird watching etc) and by whom. An audit of uses has been undertaken as part of this project across all NHS estates (see Section 2). However, each NHS Scotland Health Board will need to complete an audit of the current uses of the greenspace and the users. In order to value the benefits that flow from the greenspaces it is important to understand the number of people associated with each use type. For example, how many visitors use the footpaths, sit on the benches in nature and take part in therapeutic gardening.
An audit of informal use can be completed relatively easily but will need to be surveyed throughout the year to understand the impacts of factors such as weather on use. This can be combined with the zoning idea outlined above, where a survey can focus on the number, type of people and use in the different zones around an estate site. Specific green health interventions organised on site should be registered to help the NHS board identify uses and to record the numbers of participants involved in the activity. In terms of measuring the numbers of people involved in more general recreation activities such as using the estate for cycling, walking to work, walking for leisure etc, tech could be designed for innovative ways of measuring use. Counters can be used on footpaths and cycle paths, sensors on benches, innovative smartphone apps (GPS location data can also be captured by volunteers (Ladle et al., 2018)) could be used in association with citizen science projects. The methods of data capture possible will differ depending on the type of activity and beneficiary group.
Benefits
Health and well-being benefits from cultural services
There will be numerous benefits flowing from greenspace use and to value these benefits it is important to collect data on the health and well-being outcomes. The review of the metrics for the valuation of health and well-being benefits (Section 4 above) has revealed that there are a wide range of benefits (Table 7 & 8) and approaches to measuring these in the scientific literature. These range from mental health or well-being benefits such as decreases in depression and anxiety and increased social cohesion, to physical health benefits such as lower blood pressure and increased cardio-vascular health. A choice has to be made as to which benefits will be measured. The valuation method to be used needs to be decided first as this influences the way the data should be collected. It is important that the right method is applied to the right activity. The literature review also demonstrated the wide range of valuation methods that can be applied and nested together (Table 8). To complicate matters, in reality, there may be more than one benefit type flowing from the use of the greenspaces, for example, walking in a greenspace may increase physical health, mental health and social cohesion. The CCA in Step 1 and the SROI approach in Step 2 of the proposed framework are designed to identify these complexities and a decision can then be made as to what needs to be measured and what valuation method is most appropriate, using the Green Book (HM Treasury, 2021) as a benchmark. Using a mix of valuation methods to suit different situations is important.
Issues with benefits transfer
There is a requirement for primary data collection to understand the uses and benefits associated with the NHS greenspace beneficiaries, rather than using existing studies for benefits transfer. Some of the existing metrics for measuring physical and mental health benefits associated with visits to greenspaces are used as benefits transfers. An example of a metric that is frequently used as a benefits transfer for the valuation of (non-specific) physical health benefits from recreation in greenspace (White et al., 2016). The metric is the proportion of people who have met national physical health guidelines which is based on national level surveys of greenspace use, and the value of the QALY. These are often applied to slightly smaller scales (e.g. county scales), but are not suitable at the scale of the NHS outdoor estate, where habitats are not as diverse (there can be a limited range of habitats in these urban settings), and use will be different to that of the general population if it is applied to patients and the NHS workforce. However, benefits transfer may be appropriate for specific green health interventions, such as therapeutic gardening, where activities and beneficiaries are similar, and take place at a comparable scale. This was one approach used in the valuation of the health and well-being benefits from the NHS Lothian outdoor estate (Holt et al., 2021). Whether benefits transfer is suitable for valuation in specific contexts will be assessed as part of the CCA and SROI process in Steps 1 and 2 of the proposed framework.
The importance of primary data
It is important to start to collect primary data at the NHS estates, viewing them as natural experiments (Deidda et al., 2019). In health economics more generally there is an acknowledgement of the need to move away from economic evaluation alongside clinical trials in public health and prevention interventions and take up opportunities for economic evaluation alongside natural experiments. In the context of NHS greenspace use there is not always a control group (e.g. a group that has not experienced health and well-being benefits from use of a particular greenspace) and we have to make the best counterfactual of what would have happened, sometimes using a waiting list control (a group that will experience benefits from use of a particular greenspace but at a later time) or matched comparative group (a group that has roughly the same health and well-being issues before access to greenspace, as those with access to it). Given this it is important when promoting a new activity or area of greenspace (an intervention) on an NHS estate, to be prepared to collect data before and after the intervention. Simple things like footfall and the use of qualitative feedback from staff, patients and the public can be captured by survey, as well as working with academic and consultancy partners to design more complicated preference-based experiments and evaluations.
Stated preference valuation
Stated preference valuation is a group of techniques which use the individual respondents’ statements about their preferences to estimate change in utility or well-being associated with a proposed increase in quality or quantity of an ecosystem service. Through a carefully designed questionnaire choices can be presented to people, usually a specified change compared to a baseline situation. This means finding out peoples’ preferences and willingness to pay for particular benefits. These can be designed as Contingent Valuation experiments which will ask direct Willingness to Pay or Willingness to Accept questions, or choice modelling which involves different options with different costs and asking the respondent their preference. This establishes what people say they prefer, but what people actually do may be different, which is where this method invites criticism. These preference statements need to be complemented by observational studies of what people are actually doing in NHS outdoor estates. We advocate working with experts in the field of health economics, natural ecosystems and in Universities and consultancies to ensure that evaluation becomes research which can be published in peer-reviewed journals, widening impact as well as the need for dissemination in an accessible format to stakeholders. This may be in the form of videos, infographics, animations and newsletters on websites.
The travel cost method
Another method that may be useful for valuing the recreational benefits of the NHS estate is the Travel Cost Method. How much people spend on travelling (fuel, food) to a greenspace can be observed. What they pay in travel is a reflection of how much the recreational trip is valued. Again, we recommend working with experts in the field in universities and consultancies to generate high quality evidence for the design of future use of the NHS green estate.
An annual survey of well-being related to greenspace
Understanding the benefits and their value is, therefore, contingent on gathering data by survey. A well designed annual survey of well-being related to greenspace is recommended. This should also be used to gather important data on the users, such as user type (patient, staff, visitor or local user), gender, ethnicity and socio-economic circumstances. Spotting the gaps in users will enable NHS Boards to take appropriate action to establish equality of accessibility.
Health and well-being benefits from provisioning and regulating services
The health and well-being benefits associated with the provisioning and regulating services can be captured using benefits transfer as in natural capital accounting. A good guide for economic methods is provided in the Defra ENCA ecosystem services data book (DEFRA, 2020).
6.2. Where to start?
Capturing the value of all the possible health and well-being benefits, across all activities and beneficiaries associated with NHS Scotland’s outdoor estate will be challenging. Consequently, it is sensible to focus initially on using the proposed framework to evaluate situations where there are relatively easy wins, while data is gathered for dealing with the rest. There are a number of possible ways of doing this, for example, focussing on the main uses (or those considered a priority across all of the NHS Health Board estates, based on results from the survey of uses (see Section 2)), choosing activities where there is likely to be more data available or where value/benefits transfer will be possible, or focusing on a particular activity or beneficiary group where improvements to greenspace use or access to activities could have the most social and economic impact.
Health and well-being benefits for NHS Scotland staff
A major beneficiary of access to quality greenspace on site could be the NHS Scotland’s own workforce. NHS Scotland employed just under 182,000 people in 2022 (NHS Education for Scotland, 2022). Absence through sickness is an issue generally in the NHS and last year the sickness absence rate was 5.7%, the highest for a decade. This recent increase is likely to do with the health and well-being impacts on staff of the COVID-19 pandemic, but is also likely to be a consequence of an NHS system under strain.
The NHS in Scotland recognises through its Climate Emergency and Sustainability Strategy (Scottish Government, 2022a) that it can “contribute to the foundations of community health particularly through providing health-promoting environments.”. This should also apply to its own workforce, and managing the outdoor estate so it is accessible in a way that meets staff needs is key. A survey of staff use of the outdoor estate in and out of working hours (how many use it and which areas they use) at a hospital such as Forth Valley Royal would be a good place to start, and depending on the outcome a further survey to consult staff about their greenspace needs on site, along with measures to ensure working cultures to promote regular breaks outside are promoted.
A focus on the value of the health and well-being benefits of staff use of the NHS outdoor estate could establish what the baseline value is now, and as part of Step 2 of the proposed framework (SROI) test a scenario for an increase in the number of staff benefitting. The impacts are likely to be wide ranging, particularly in decreasing absenteeism, and retaining and attracting new staff, and creating resilience for future pandemics. The economic value is also likely to be high.
The annual survey of well-being related to greenspace proposed above, should be created for NHS staff as well as other beneficiaries.
Focus on mental health
A focus on mental health may be advantageous initially. The literature review demonstrated that there are numerous scales for collecting data on mental health and well-being (e.g. Warwick Edinburgh Mental Well-being Scale and the Perceived Stress Scale) that could be employed within step 2 of the proposed framework. ICECAP is an example of a set of well-being measures specifically designed for use in economic valuation and linked to the ‘capability approach’ that defines well-being in terms of an individual’s ability to do and be the things that are important in life. There are measures for adults, older people, and care-related well-being measures. These can be used before and after an activity in greenspace to understand the impact of that activity or interventions on self-reported well- being. Once this change in well-being has been established it is possible to value the change in well- being by mapping it onto a QALY, or using a well-being adjusted life year (WELLBY) which has a recommended standard value (£13,000) (see Green Book (HM Treasury, 2021)). The next step might be to focus on physical health assessments.
Specific green health interventions
There were a number of studies in the review (Section 4), that were identified as using benefits metrics and valuation metrics, focused on measuring and valuing the benefits of gardening and therapeutic gardening programmes. These have used SROI as in our proposed framework. If there is a desire to focus on health and well-being benefits flowing to patients, then these activities may be a good place to start. Social and green prescribing may also be a good focus initially, if these schemes are used within the NHS Health Boards, and the patient is using, or has the opportunity to use, the outdoor estate for their prescribed activity.
Demonstration or pilot sites
The proposed framework needs to be tested. A set of NHS Health Boards should be chosen to pilot the framework. The NHS Greenspace Demonstration Project sites and the four Green Health Partnership pilots could be used to evaluate and value the mental health benefits of the NHS workforce’s use of the outdoor estate. A workforce survey could be used at the main hospital sites to understand greenspace need and current use. A number of activities / interventions could be suggested to meet these needs, then it would be possible to begin valuing the benefits. There may be a focus on different user groups or specific activities at the other pilot estates, so a broader learning can be rolled out to other NHS Scotland Health Boards. NHS Scotland need to build a strategy that prioritises the ‘experiments’ they would like to trial.
A key policy is to reduce health inequalities across local communities, so this should be a focus at least one of the pilot estates. The Joseph Rowntree Foundation Progressive Framework (Joseph Rowntree Foundation, 2022) for harnessing the power of anchor institutions should be used as a self-assessment and decision support tool at one, and then eventually all Health Boards, to work towards becoming an inclusive anchor organisation. In addition, each NHS Health Board can use the Public Health Scotland Place and Wellbeing Outcomes and the Public Health Scotland Place Standard tool to aid decision-making and progression within the place-based building blocks framework for the evaluation, valuation and enhancement of health and well-being benefits for all across the NHS outdoor estates.
Funding and multi-agency collaborations
All interventions in the outdoor estate should have an evaluation budget associated with them so the proposed framework can be followed, and the value of the investment can be estimated. Funding will always be an issue. However, a relatively small investment in a full time staff member to champion the benefits from greenspace at each Health Board would mean that planning, organisation, data gathering and monitoring could be put in place.
Multi-agency collaboration is key to funding and delivering programmes/activities/interventions that will bring improvements in well-being. This could be with third sector, public and private sector organisations that have the same goals. The volunteer resource could also be used to help gather data and set up programmes. For example, the Royal Voluntary Service could take patients out in greenspace, which is particularly important in hospice care.
Providing incentives to the Health Boards for reaching certain goals may also help. There might be a site or estate level award for the best health and well-being provision, or a recognition scheme based on the achievement of set levels (e.g. bronze, silver and gold).
7. Conclusions and recommendations
This project conducted a survey of the uses of the NHS Scotland outdoor estate that captured the extensive range of uses which already exist within the outdoor estate. The survey findings suggest that there is a great deal more which could be done with the estate for therapeutic and well-being benefits, that there is some awareness of this potential and an enthusiasm to develop the use of the estate in this way. Awareness of the potential is not, however, universal and there is scope to raise the level of awareness of the potential which is clearly there amongst some users.
This aspiration could be supported by greater recognition of this potential in health and treatment pathways and protocols, and specific inclusion within Property and Asset Management Strategies (PAMS). It may be possible to tackle obstacles which arise from existing demands on staff by working more collaboratively with external organisations, and within the NHS itself.
A logic chain (Figure 3) made explicit the relationships between the natural capital assets, final ecosystem services and the health and well-being benefits of the NHS outdoor estate. It demonstrated that there are many factors, such as size, type, spatial location, quality and accessibility of greenspace that will influence activity, and the frequency and time spent in greenspace will impact on the level of well-being benefits received. This conceptual model should be used to guide the NHS Health Boards in identifying what needs to be measured for the eventual valuation of benefits. It can also form the basis of a future valuation toolkit that integrates environmental and health and well-being benefits (but see Section 8 below).
The literature review revealed many studies that quantify the mental health and physical health benefits of greenspace use. However, there are relatively few studies that have valued the health and well-being benefits derived from activities in greenspace. The studies that have done so have used a range of valuation methods (outlined in Table 10 below). The review documented the metrics and values used in the studies so benefits transfers can be used where it is appropriate (see Table A2 in the Appendix 2). Natural capital toolkits were also reviewed (Table 10) and it was concluded that no one toolkit will be useful for valuing the health and well-being benefits. Indeed, many of the toolkits specialise in valuing a range of benefits, not just health and well-being ones, but specific models or approaches within them may be taken and applied to certain uses of the NHS outdoor estate, rather than using the toolkits themselves.
| Methods used for valuing physical and mental health benefits in studies identified in the rapid review | Natural capital toolkits that provide useful metrics to value health and well-being benefits |
|---|---|
| Quality adjusted life year (QALY) | Health Economic Assessment Tool (HEAT) |
| Disability adjusted life year (DALY) | Environment Valuation Online (NEVO) |
| Cost benefit analysis (CBA) | Outdoor Recreation Valuation (ORVal) |
| Value of a statistical life (VOSL) | InVEST |
| Travel cost method (TCM) | iTree Eco |
| Contingent valuation (CVM) and Willingness to pay within this (WTP) | Green Infrastructure Valuation Toolkit (GI-Val) |
| Health adjusted life year (HALY) | Co$ting Nature |
| Cost-effectiveness analysis (CEA) | Benefits Estimation Tool (B£ST) |
| Discrete choice experiment (DCE) | Greenkeeper |
| Social Return on Investment (SROI) | - |
Emerging from the consultation with three experts in health economics, we have proposed a three step standardised and modular (building blocks) framework to apply to the evaluation and valuation of benefits flowing from NHS Scotland’s outdoor estate. We have been able to outline the data required to begin on the journey towards valuation of the benefits, and suggest some areas of focus that might have the greatest impact in the short term, whilst preparing to value the rest of the benefits in the medium to long term.
Two important conclusions have emerged from this work:
- There is no quick route to valuing the health and well-being benefits of the NHS outdoor estate in a robust way. There may be some quick wins using benefits transfer from other studies for specific organised health activities where there are known numbers of participants, or from very generic recreational activities in specific habitats (such as walking in woodland). However, the latter would still need data on the number of people involved in these activities.
- Primary studies using surveys will be necessary to quantify and value health and well-being benefits across a range of NHS outdoor estate activities. The most efficient use of resources would be to prioritise certain activities or user groups and run different projects on pilot NHS Health Board sites. The learning can then be applied to other sites and be used as part of a valuation toolkit in the future.
Given this the following recommendations will lead to a robust evaluation and valuation of the health and well-being benefits from the use of the NHS outdoor estate. They will also help NHS Scotland develop their role as an anchor institution, allowing the outdoor estate to contribute to prevention of illness and address health inequalities:
Adopt a place-based approach with an awareness of the opportunities being different for urban and rural estate: aligning with the anchor institution concept and the NHS Scotland Climate Emergency & Sustainability Strategy, so the NHS outdoor estate can be managed to influence the social, economic and environmental factors that help create good health, playing a key role in addressing health inequalities for patients, NHS staff and the local community.
Awareness of time-horizons for valuation and the role of discount rates: Both the Treasury and National Institute for Health and Care Excellence (NICE, 2012 and 2013) have recommendations for the use of differential discount rates for preventative interventions which are relevant to the evaluation of the green estate and activities that promote health and well-being across provisioning, regulating and cultural ecosystem services. It is advisable that a range of discount rates are used in any analysis along with different time-horizons (e.g. 3 years, 10 years, 20 years).
A shift in thinking about hospitals and their estate as places of acute care to places with a role to play in prevention: ensure that the NHS Scotland shifts towards preventing ill health rather than just treating it. Measures are required to ensure a broadening of decision-makers and medical professionals perspectives to think in terms of prevention.
Begin to gather data and monitor use of the green estate: across the natural capital assets of the outdoor estate (including habitat quality and accessibility), the final ecosystem services (the activities taking place within the natural capital assets and by whom), and the benefits from the cultural services as well as the provisioning and regulating services. This requires an audit of outdoor estate uses, a register of green health interventions occurring on site, monitoring of the number of people using the outdoor estate across different activities at different times of the year, and an annual survey of health and well-being related to outdoor estate use.
Employ the proposed building blocks framework to valuation: use the standardised and modular approach for the evaluation and valuation of the health and well-being benefits flowing from the NHS outdoor estate. Recognise that there are a broad range of values both health and non-health and that this requires both qualitative and quantitative approaches. Use the CCA (Step 1) to list the costs and impacts and to think about appropriate methods of valuation, use SROI (Step 2) and a mixed methods approach to ensure the right method of valuation for the right activity using the HM Treasury Green Book as a benchmark (for health and well-being benefits from cultural services, and integrating standard natural capital accounting valuation methods for these benefits from provisioning and regulating services). Use MCDA (Step 3) for the prioritisation of options at the NHS Health Board estate scale.
A focus on benefits to the NHS workforce, on mental health and musculoskeletal health: the health and well-being benefits flow from a diversity of activities within the outdoor estate and across a range of beneficiaries. Focusing on the NHS workforce is a good place to begin the evaluation and valuation of benefits from the outdoor estate. A SROI for increasing the well-being of staff, decreasing absenteeism and workforce resilience through improved access, and opportunities to access, greenspace is likely to demonstrate a good return. A focus on mental health benefits is another way of narrowing the challenge down. There are a number of established methods for measuring mental health benefits from activity in greenspace, and this could be married with the NHS workforce focus. A patient focus could also begin with therapeutic gardening.
Establish the concept of zoning the green state for staff, for patients and visitors, for green parking such as that set out in Urban Blue Green Grids guidance, and for community activities using green estate land: for example, walking, cycling, gardening, playgrounds, arboreta etc.
Establish demonstration sites with built-in evaluation and the resources to deliver it, with outside links to those familiar with evaluation methods of costs and benefits: to pilot the proposed framework. These could be the Green Health partnership sites, NHS Greenspace Demonstration Project sites or other NHS Health Boards. One approach could be to pick hospital sites with contrasting areas of outdoor estate, to test the health and well-being impacts of greenspace use, for example, the Western General in Edinburgh (very little greenspace) and the Forth Valley Royal (a large outdoor estate). Focus initial efforts to value the health and well-being benefits on the workforce at these sites, or pick a different focus for each and roll out the learning to other sites.
Delivering evaluations including academic publication in peer-reviewed journals as well as accessible web-based reports and infographics: all interventions should have an allocated evaluation budget. A member of staff dedicated to championing the evaluation of the benefits from the outdoor estate at each Health Board is required. Multi-agency collaboration and the use of volunteers can help with funding and improving access of beneficiaries to the outdoor estate.
Working collaboratively with experts in the field: we recommend working with experts in the field in universities and consultancy firms to generate high quality evidence for the design of future use of the NHS outdoor estate.
8. Next steps
The goal of this NatureScot and Public Health Scotland commissioned project was to develop a conceptual model for a toolkit (a GIS based or natural capital accounting type tool or set of tools), that could be used to value the health and well-being benefits from the NHS outdoor estate. The logic chain model (Figure 3, Section 3), relating the natural capital assets of the NHS outdoor estate to provisioning, regulating and cultural services that in turn give rise to the health and well-being benefits that can be valued is this conceptual model. The creation of the tool was to be phase 2 of the project. The development of a tool is still possible, but this should be a medium to long term ambition. The aspiration should be to initially include in a tool activities where benefits can be valued by benefits transfer from the scientific and grey literature now (this applies to specific green health activities as discussed above, but also to the regulating services such air pollution regulation and local climate regulation), then the tool can be added to in the medium to long term using benefits transfer from data on primary studies carried out across NHS estates focused on particular activities or user groups. This would produce a more robust tool. The long term goal should be to prioritise a set of activities common to all NHS Health Board estates that can be fully valued, so that the resultant valuation, although still incomplete, would go some way to quantifying a large proportion of the value of the health and well-being benefits provided across the NHS Scotland estate.
The next stage for this project should be to focus on setting up the baseline data required (as outlined in Section 6 and the above recommendations) for valuations, along with a range of projects across activities and users at pilot NHS Health Board estates. Alongside this there should be a strategic plan or policy for the delivery of these projects across the NHS Health Boards and staff responsible for delivering it.
References and Appendices
References
Cheshmehzangi, A. 2022. Vulnerability of the UK’s BAME communities during COVID-19: The review of public health and socio-economic inequalities. Journal of Human Behavior in the Social Environment, 32(2), 172-188.
Cronin-de-Chavez, A., Islam, S. and McEachan, R.R. 2019. Not a level playing field: A qualitative study exploring structural, community and individual determinants of greenspace use amongst low-income multi-ethnic families. Health and Place, 56, 118-126.
Dawkins, T.R.T. 2022. Making cities green. Understanding willingness to pay (WTP) for components of green spaces within urban communities: A discrete choice experiment. Kent Economics Undergraduate Research Journal Vol 1.
Deidda, M., Geue, C., Kreif, N., Dundas, R. and McIntosh, E. 2019. A framework for conducting economic evaluations alongside natural experiments. Social Science and Medicine, 220, 353-361.
DEFRA, 2020. Enabling a Natural Capital Approach (ENCA).
Edwards, R.T. and Holt, A. 2023. Building blocks for evaluation – public health economics.
Edwards, R.T. and Lawrence, C.L. 2021. ‘What You See is All There is’: the importance of heuristics in cost-benefit analysis (CBA) and social return on investment (SROI) in the evaluation of public health interventions. Applied Health Economics and Health Policy, 19(5), 653-664.
Edwards, R.T. and McIntosh, E. 2019. eds. Applied health economics for public health practice and research. Oxford University Press.
Edwards, R.T. 2022. Well-being and well-becoming through the life-course in public health economics research and policy: A new infographic. Frontiers in Public Health, 10.
Fujiwara, D. 2014. Measuring the social impact of community investment: the methodology paper. London, England: Housing Associations Charitable Trust (HACT).
Fujiwara, D. 2015. The seven principle problems of SROI. London, England: Simetrica Ltd.
Greenspace Scotland, 2022. Open space strategy and play sufficiency assessment draft regulations report of health inequalities impact assessment scoping exercise.
H.M. Treasury, 2022. The Green Book.
Haines-Young, R. and Potschin, M. 2018. Common International Classification of Ecosystem Services (CICES) V5.1. Guidance on the application of the revised structure. Fabis Consulting.
Hinde, S., Bojke, L. and Coventry, P. 2021. The cost effectiveness of ecotherapy as a healthcare intervention, separating the wood from the trees. International Journal of Environmental Research and Public Health, 18:11599.
Holt, A.R., Dempsey, N., Henneberry, J.M., Ashby, M. and Lush, C. 2021. Biodiversity and climate change assessment for the NHS Lothian estate. Report to the NHS Lothian, Natural Capital Solutions Ltd, February 2021.
Hutchinson, C.L., Berndt, A., Forsythe, D., Gilbert-Hunt, S., George, S. and Ratcliffe, J. 2019. Valuing the impact of health and social care programs using social return on investment analysis: how have academics advanced the methodology? A systematic review. British Medical Journal Open, 9, e029789.
Joanna Briggs Institute, 2017. Critical Appraisal tools for use in JBI Systematic Reviews.
Joseph Rowntree Foundation, 2022. Harnessing the power of anchor institutions – a Progressive Framework.
Ladle, A., Galpern, P. and Doyle-Baker, P. 2018. Measuring the use of green space in urban resource selection function: An application using smartphone GPS locations. Landscape and Urban Planning, 179, 107-115.
Marmot, M. 2020. Health equity in England: The Marmot review 10 years on. British Medical Journal, 368.
Mercer, T. and Lacy, P. 2021. A brief introduction to realist evaluation. Public Health England.
Millennium Ecosystem Assessment, 2005. Ecosystems and human well-being: Synthesis. Island Press, Washington D.C.
National Institute for Health Research, 2018. Cost-consequence analysis: An underused method of economic valuation.
New Economics Foundation Consulting, 2020. Social return on investment.
NHS Education for Scotland, 2022. NHS Scotland Workforce: Latest statistics at 21st March 2022. An Official Statistics publication for Scotland, 7th June 2022.
NICE, 2012. Methods for the development of NICE public health guidance (third edition).
NICE, 2013. Guide to the methods of technology appraisal 2013.
Natural Capital Committee, 2014. The state of natural capital: Restoring our natural assets. Second report to the Economic Affairs Committee. Natural Capital Committee, March 2014.
Nicholls, J., Lawlor, E., Neitzert, E. and Goodspeed, T. 2012. A guide to Social Return on Investment. The SROI Network.
Nicholls, J., Lawlor, E., Neitzert, E. and Goodspeed, T. 2009. A guide to social return on investment. Office of the Third Sector, Cabinet Office.
Oliveira, M., Mataloto, I. and Kanavos, P. 2019. Multi-criteria decision analysis for health technology assessment: addressing methodological challenges to improve the state of the art. The European Journal of Health Economics, 20, 891-918.
Olsen, J.R., Nicholls, N., Panter, J., Burnett, H., Tornow, M. and Mitchell, R. 2022. Trends and inequalities in distance to and use of nearest natural space in the context of the 20-min neighbourhood: A 4-wave repeat cross-sectional study, 2013-2019. Environmental Research, 213, 113610.
Public Health Scotland, 2022. Evidence behind the Place Standard Tool and Place and Well-being Outcomes.
Reed, S., Göpfert, A., Wood, S., Allwood, D. and Warburton, W. 2019. Building healthier communities: the role of the NHS as an anchor institution. The Health Foundation.
Skivington, K., Matthews, L., Simpson, S. A., et al. 2021. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. British Medical Journal, 374.
Scottish Government, 2016. The Procurement (Scotland) Regulations 2016.
Scottish Government, 2021. A fairer, greener Scotland: Programme for Government 2021-22.
Scottish Government, 2022a. NHS Scotland Climate Emergency and Sustainability Strategy 2022-2026.
Scottish Government, 2022b. Care and Wellbeing Portfolio Board.
Scottish Government, 2022c. Local living and 20 minute neighbourhoods, Chapter 15 National Planning Framework 4.
Thokala, P. 2011. Multiple criteria decision analysis for health technology assessment. School of Health and Related Research (ScHARR), University of Sheffield.
The Scottish Parliament, 2022. Proposed Well-being and Sustainable Development (Scotland) Bill.
White, M.P. et al. 2016. Recreational physical activity in natural environments and implications for health: A population based cross-sectional study in England. Preventative Medicine, 91, 383-388.
Willings, B. 2017. A broader economic evaluative space for public health interventions: an integrated approach. PhD thesis, University of Glasgow.
Wong, G., Greenhalgh, T., Westhorp,G., Manzano, A., Greenhalgh, J. and Jagosh, J. 2016. RAMESES II reporting standards for realist evaluations. BMC Medicine, 14.
Appendix 1. Review protocol
The review was guided by the conceptual model/logic chain outlined in Section 3 of the main report. A rapid evidence review/assessment methodology was used. Rapid evidence reviews are used in health sciences by Defra and in reviews commissioned by the Scottish Government. We drew on good practice from the Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews (Joanna Briggs Institute, 2017). We outline the protocol that was used below:
i. Inquiry question
The aim of the review was to find studies that contain metrics/toolkits for quantifying the health and well-being benefits derived from activities in greenspaces related to the NHS outdoor estate. The following questions guided the review:
- What are the health and well-being benefits from exposure to greenspaces of the type found on NHS estates? (Benefits delivered via regulating services and cultural services.)
- What are the health and well-being benefits from specific health interventions (activities) employed by the NHS estates? (Benefits delivered via regulating services and cultural services.)
- How are physical flow of benefits quantified? (Toolkits used or individual metrics.)
- How are the monetary values of these benefits quantified? (Toolkits used or individual metrics.)
The review focused specifically on studies that quantify the relationships between the greenspace type (e.g. park / allotment / woodland) or intervention (e.g. green gym, therapeutic gardening) and the health and well-being response to exposure or participation (e.g. decrease in stress, increased quality of life, reduced mortality or morbidity).
ii. Inclusion criteria
The focus was on studies from the natural capital and health economics literature. International studies in English were included if they are appropriate to the context. Studies needed to include single metrics or toolkits that aim to quantify these relationships from grey or primary literature between 2000-2022.
The focus was initially on systematic, narrative and literature reviews and robust primary evidence. There were a number of key reviews to include:
WHO, World Health Organization, Regional Office for Europe, 2016. Urban Greenspaces and Health: A Review of Evidence, WHO, Copenhagen.
WHO, World Health Organization, Regional Office for Europe, 2017a. Urban Greenspace Interventions and Health: A Review of Impacts and Effectiveness, WHO, Copenhagen.
WHO, World Health Organization, Regional Office for Europe, 2017b. Urban Greenspaces: a brief for action, WHO, Copenhagen.
Maxwell, S. and Lovell, R. 2017. Evidence Statement on the links between natural environments and human health, DEFRA, London.
Lovell, R., Depledge, M. and Maxwell, S. 2018. Health and the natural environment: A review of evidence, policy, practice and opportunities for the future, DEFRA, London.
Lovell et al. 2020. A rapid scoping review of the health and well-being evidence for the Framework of Green Infrastructure Standards. Natural England.
iii. Search strategy
The searching was iterative and search terms (as outline below) were combined. Searches were conducted using key academic databases including PubMed, PsycINFO, Scopus, and Web of Science. An internet search using Google and Google scholar was also included to capture grey literature. Citation searches were important when key papers have been identified. The search terms used are outlined in Table 6 of the report.
iv. Selection process
All articles from the search were filtered first by title and if any obviously irrelevant studies (i.e. they are not relevant to the rapid review questions and do not quantify the relationships between greenspace/intervention and health and well-being outcomes) were rejected. If the title was relevant, it was filtered by abstract. If the abstract was appropriate the whole article was accepted for review.
v. Critical appraisal
The quality of the study was determined once accepted. An evidence schedule documenting the title of the study, source, description, and study type (e.g. quantitative Social Return on Investment, economic (valuation, cost-benefit), and primary research or secondary study / benefits transfer) was created. It provided a short narrative overview of the topic, highlighting what is known and commenting on the nature of the evidence base with an overview of strength/weakness and gaps. Each study was then scored (high, medium, low) according to quality and robustness which was judged according to the following criteria:
- Specific questions and hypotheses have been addressed
- Related to existing research or theories,
- Measurements and analytical techniques are appropriate and robust,
- Conclusions are backed up by well presented data and findings
- Assumptions and limitations have been discussed.
vi. Results
The most suitable high quality studies were chosen and taken through for discussion with the expert panel to identify whether further searching is required.
vii. Synthesis
A narrative report which highlights key findings from the evidence was created (see Section 4 of the main report).
Using this approach, we aimed to present a fair interpretation of the evidence base. However, while we initially prioritised any systematic reviews, meta-analyses and robust primary evidence, these were in relatively short supply. This is due to the nature of measuring health and well-being benefits (it is challenging to quantify health and well-being benefits and estimate non-market values) which means it is not possible to complete randomised controlled trials within this context, so what is viewed to be the ultimate in robust evidence is not attainable in this context (as discussed in Section 5 of the main report).
Appendix 2. Rapid review valuation metrics summary
Table A2. Summary of papers valuing the health and well-being benefits of activities in greenspace including greenspace type, benefit type, valuation methods used, valuation results (£), quality assessment (L = low, M = medium, H = high) and paper/report reference (there is a full reference list below the table). Please note that an Excel file has also been made available to the project team outlining the below information organised by study.
| Greenspace | Benefit | Valuation measures | Value results | Quality | Papers |
|---|---|---|---|---|---|
Active travel/trails | General health (n=2) | DALY (as part of a CBA) x1 Cost analysis x1 | Cost per user: $235; saving per user: $622 Net gain of NZ$151.2 m | M x2 | Chapman et al Wang et al |
| Bluespace | Recreation (n=2) | Policy framework x1 Travel cost model x1 | Average cost to visit a river: $128 - $393 Lake closures cause net loss of $1,274 - $37,030 per day | M x1 L x1 | Rabinovici et al Smith and Moore |
| Garden/ allotment | Well-being (n=2) | SROI x2 | £3 return for every £1 invested £3.56 return for every £1 invested | L x2 | Pank et al Schoen et al |
| Greenspace other |
Education (n=1) | Boost in lifetime earnings and enhancement of future QoL | Nature-based school trips to reserves: £850,000 - £1.3m (national) Participation in Big School Birdwatch: £188 per school |
L x1 |
Mourato et al |
| Greenspace other | General health (n=2) | QALY x1 HALY (within CBA) x1 | £6414 - £21,519 per QALY Healthcare savings due to prevented physical activity-related diseases: A$3,100 – A$105,355 per 100,000 adults per yr |
L x2 | Mourato et al Zapata-Diomedi et al |
Greenspace other | Mental health (n=1) | QALY | USD 100bn contribution to Aus (population estimate 20 mil so per capita = 5000) | M x1 | Buckley et al |
Greenspace other | Physical activity (n=1) | QALY | £2.18 billion per yr (England) | M x1 | White et al |
| Greenspace other |
Recreation (n=2) |
Meta-analysis x2 | £3.35 per trip £3.59/person/visit to woodland and forest £1.82/person/visit to freshwater and floodplain |
M x2 | Sen et al 2012 Sen et al 2014 |
| NBI | General health (n=2) | Benefit-cost ratio x1 SROI x1 | SROI of £6.88 - £8.50 for every £1 invested Benefits from reduced public service use per person: £830 - £31,520 per yr | M x2 | Bagnall et al Pretty and Barton |
| NBI | Mental health (n=1) | Avoided public sector costs | Avoided cost between £4,151 and £12,799 | L x1 | Vardakoulis |
| NBI | Well-being (n=1) | QALY | Cost per QALY: £8,600 per yr | L x1 | CJC Consulting |
Urban greenspace | Recreation (n=1) | TCM WTP | $1,186/ha/yr (WTP) $15,440/ha/yr (TCM) | M x1 | Lupp et al |
Urban greenspace | Well-being (n=1) | WTP | €23 to increase green urban areas €455 to decrease distance between households and green areas by 100m | M x1 | Krekel et al |
| Walking | General health (n=3) | HEAT Tool x1 Discrete choice experiment x1 QALY x1 | £3.5m/yr saved in prevented deaths directly attributed to Wales Coastal Path Walking to Health Initiative over 3 years provides £4008.98 per QALY Increased walkability and perception of access = increase by £13.56/person/week | M x1 L x2 | Cavill et al Longo et al Stone |
| Woodland | General health (n=1) | Health effect value | £900,000 per year (national) | M x1 | Powe and Willis |
| Woodland | Mental health (n=1) | QALY | Cost per person for intervention £7.68 - £11.80 | M x1 | Ward Thompson et al |
| Woodland | Recreation (n=8) | Travel cost method x2 Contingent valuation method x3 Constant value per trip x1 WTP x1 QALY x1 CEA x1 | (Forest recreationalist WTP) avoid postponement = 7.57 SEK; not lose health benefits = 17 SEK £9.75 - £18.50 per visit (2014) £2.69 - £13.45 per trip (2014) €12.33 per visit Individual WTP = €9.50 Benefit to economy = €194 Per person: £6 - £8,542 Per woodland: £2,581 - £70,832 Cost per user: £426 |
M x5 L x3 | Christie et al Doctorman and Borman Eftec Hynes et al Jankovska and Straupe Moseley et al Scarpa Willis et al |
Full reference list of studies from table A.2
Bagnall, A.-M. Brymer, E. and Southby, K. 2019. Social return on investment analysis of the health and wellbeing impacts of wildlife trust programmes.
Buckley, R., Brough, P., Hague, L., Chauvenet, A., Fleming, C., Roche, E., Sofija, E. and Harris, N. 2019. Economic value of protected areas via visitor mental health. Nature Communications, 10, 5005.
Cavill, N., Rutter, H. and Gower, R. 2014. economic assessment of the health benefits of walking on the Wales Coast Path. Natural Resources Wales.
Chapman, R., Keall, M., Howden-Chapman, P., Grams, M., Witten, K., Randal, E. and Woodward, A. 2018. A cost benefit analysis of an active travel intervention with health and carbon emission reduction benefits. International Journal of Environmental Research and Public Health, 15(5) 962.
Christie, M., Hanley, M., Warren, J., Murphy, K., Wright, R. and Hyde, T. 2006. Valuing the diversity of biodiversity. Ecological Economics, 58(2), 304-17.
CJC Consulting, 2016. Branching out economic study extension final report.
Doctorman, L. and Boman, M. 2016. Perceived health state and willingness to pay for outdoor recreation: an analysis of forest recreationists and hunters. Scandinavian Journal of Forest Research, 31, 611-617.
Eftec, 2010. The economic contribution of the public forest estate in England.
Hynes, S., Cahill, B. and Dillon, E. 2007. Estimating the amenity value of Irish woodlands. Irish Forestry.
Jankovska, I., Donis, J. and Straupe, I. 2011. Monetary value and social role of forest recreation services in Latvia. Research for Rural Development, 2, 65-70.
Krekel, C., Kolbe, J. and Wüstemann, H. 2016. The greener, the happier? The effect of urban land use on residential well-being. Ecological Economics, 121, 117-27.
Longo, A., Hutchinson, W.G., Hunter, R.F., Tully, M.A. and Kee, F. 2015. Demand response to improved walking infrastructure: a study into the economics of walking and health behaviour change. Social Science and Medicine, 143, 107-16.
Lupp, G., Förster, B., Kantelberg, V., Markmann, T., Naumann, J., Honert, C., Koch, M. and Pauleit, S. 2016. Assessing the recreation value of urban woodland using the ecosystem service approach in two forests in the Munich Metropolitan Region. Sustainability, 8(11), 1156.
Moseley, D., Connolly, T., Sing, L. and Watts, K. 2018. Developing an indicator for the physical health benefits of recreation in woodlands. Ecosystem Services, Assessment and Valuation of Recreational Ecosystem Services, 31, 420-32.
Mourato, S., Atkinson, G., Collins, M., Gibbons, S., MacKerron, G. and Resende, G. 2010. Economic analysis of cultural services. UK National Ecosystem Services Assessment Analysis Report.
Pank, H. 2011. Social return om investment (SROI) report’. Gorgie City Farm Community Gardening.
Project. Gorgie City Farm, Edinburgh and Federation of City Farms and Community Gardens.
Powe, N.A., and Willis, K.G. 2004. Mortality and Morbidity benefits of air pollution (SO2 and PM10) absorption attributable to woodland in Britain. Journal of Environmental Management, 70(2), 119-28.
Pretty, J. and Barton, J. 2020. Nature-based interventions and mind–body interventions: saving public health costs whilst increasing life satisfaction and happiness. International Journal of Environmental Research and Public Health, 17(21), 7769.
Rabinovici, S.J.M., Bernknopf, R.L., Wein, A.M., Coursey, D.L. and Whitman, R.L. 2004. Economic and health risk trade-offs of swim closures at a Lake Michigan beach. Environmental Science and Technology, 38, 2737-2745.
Sen, A., Darnell, A., Bateman, I., Munday, P., Crowe, A., Brander, L., Raychaudhuri, J., Lovett, A., Provins, A. and Foden, J. 2012. Economic assessment of the recreational value of ecosystems in Great Britain. Working Paper. CSERGE Working Paper.
Sen, A., Harwood, A.R., Bateman, I.J., Munday, P., Crowe, A., Brander, L., Raychaudhuri, J., Lovett, A.A., Foden, J. and Provins, A. 2014. Economic assessment of the recreational value of ecosystems: methodological development and national and local application. Environmental and Resource Economics, 57(2), 233-249.
Schoen, V., Caputo, S. and Blythe, C. 2020. Valuing physical and social output: a rapid assessment of a London community garden. Sustainability, 12(13), 5452.
Smith, J.W. and Moore, R.L. 2013. Social-psychological factors influencing recreation demand: evidence from two recreational rivers. Environment and Behavior, 45(7), 821-50.
Stone, D. 2009. An estimate of the economic and health value and cost effectiveness of the expanded WHI scheme 2009.
Vardakoulias, O. 2013. The economic benefits of ecominds: a case study approach. Nef Consulting Ltd.
Wang, G., Macera, C.A., Scudder-Soucie, B., Schmid, T., Pratt, M., Buchner, D. and Heath, G. 2004. Cost analysis of the built environment: the case of bike and pedestrian trials in Lincoln, Neb. American Journal of Public Health, 94(4), 549-53.
Ward Thompson, C., Elizalde, A., Cummins, S., Leyland, A.H., Botha, W., Briggs, A., Tilley, S. et al. 2019. Enhancing health through access to nature: how effective are interventions in woodlands in deprived urban communities? A quasi-experimental study in Scotland, UK. Sustainability, 11(12), 3317.
White, M.P., Elliott, L.R., Taylor, T., Wheeler, B.W., Spencer, A., Bone, A., Depledge, M.H. and Fleming, L.E. 2016. Recreational physical activity in natural environments and implications for health: a population based cross-sectional study in England. Preventive Medicine, 91, 383-88.
Willis, K., Crabtree, B., Osman, L.M. and Cathrine, K. 2016. Green space and health benefits: a QALY and CEA of a mental health programme. Journal of Environmental Economics and Policy, 5(2)163-80.
Zapata-Diomedi, B., Mantilla Herrera, A.N. and Veerman, J.L. 2016. The effects of built environment attributes on physical activity-related health and health care costs outcomes in Australia. Health and Place, 42, 19-29.
Appendix 3. Expert consultation
| 10.00 | Welcome and introductions: Alison Holt, Charles Cowap and all |
|---|---|
| 10.10 | Outline of the project and emerging findings: Literature Review – Alison Survey and structured discussions – Charles The task ahead – a tool to measure the health and well-being benefits – how far away are we? All |
| 11.00 | Short break |
| 11.10 | Cost Consequence Analysis We would appreciate your views on the strengths and limitations of CCA. It has been promoted to us as a useful tool (useful enough) where detailed quantification of outcomes is difficult. How do you see its strengths and weaknesses? |
| 11.40 | Broadening the horizon (1) The design of robust and ethical studies to assess green health benefits, to NICE Standards. Are we there or how far have we got to go? |
| 12.15 | Break for lunch |
| 1.00 | Reconvene: Broadening the horizon (2) Continuing the discussion on the design of robust and ethical studies to NICE Standards. What are the challenges and cost implications? How can they be overcome? |
| 1.15 | Work time. Please use this time to prepare a short summary of your personal views in response to the earlier sessions. Please feel free to prepare visual or other aids which we can share. |
| 2.00 | Individual participant presentations (please aim for approx. 10 mins each): Timings: Each presentation followed by 10 mins for short questions and comments. |
| 3.00 | Short break |
| 3.10 | Plenary – agreeing the messages which need to emerge from the day. The key action calls to:
|
| 4.00 | Close and disperse |






